 Written by Jay Campbell
Written by Jay Campbell



It’s not every day you get to be at the forefront of a brand new therapeutic peptide being released into the world.
I’ve had the privilege over the past year of covering numerous Golden Age agents for every facet of your health.
Whether it’s Ipamorelin for fat loss or Dihexa for cognitive repairment, I’ve talked about nearly all of them in great detail.
But I want to talk about a brand new peptide that JUST got released by BioLongevity Labs: KPV.
It’s the smallest peptide I’ve seen yet its size is not a reflection of its powerful health benefits… ESPECIALLY for the chronically inflamed.
Get ready to discover a brand new Golden Age treatment very few peptide physicians even know about in 2021.
What Is KPV Peptide?
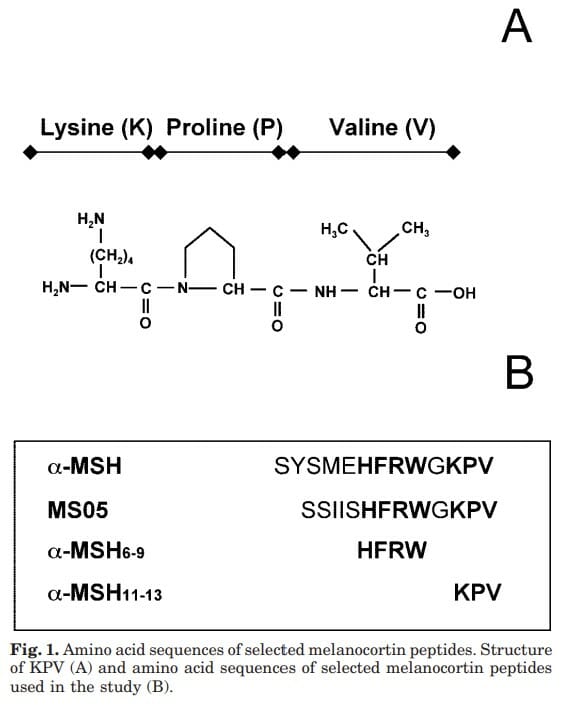
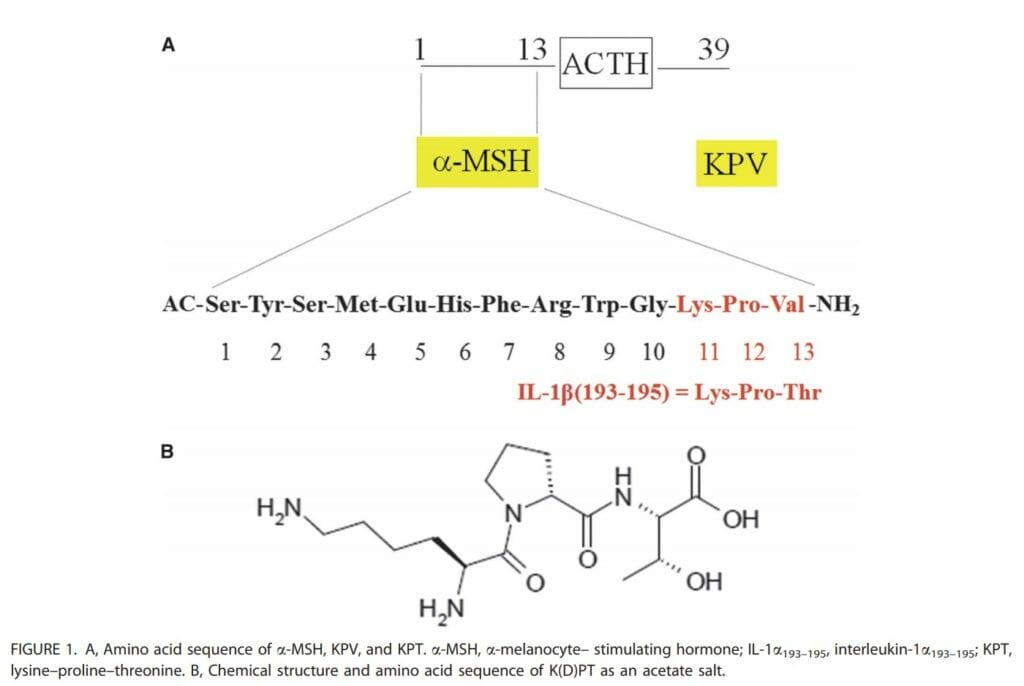
KPV is a tripeptide (i.e. 3 amino acids long) that makes up the C-terminal end of a larger naturally occurring melanocortin peptide hormone in your body known as alpha-melanocyte-stimulating hormone (α-MSH).
(Source)
Regular readers of my website will immediately recognize α-MSH because the therapeutic peptides Melanotan I and Melanotan II are synthetically derived from it.
And while α-MSH is very well-known for its anti-inflammatory effects in the human body, its major downfall is that it also does a lot more:
“The anti-inflammatory effects of α-MSH can be elicited via melanocortin receptors (MC-Rs) broadly expressed in a number of tissues ranging from the central nervous system to cells of the immune system and on resident somatic cells of peripheral tissues. α-MSH affects various pathways regulating inflammatory responses such as NF-κB activation, expression of adhesion molecules, inflammatory cytokines, chemokine receptors, T-cell proliferation and activity and inflammatory cell migration
“A broad range of effects of α-MSH exerted beyond the field of inflammation, its pigmentory capacity being only the most visible aspect, has been one of the major impediments limiting the use of α-MSH in human inflammatory disorders“
In other words, you would fix inflammation but at the cost of getting a darker skin tan, which happens due to the stimulated release of melanin (the skin-darkening pigment) by cells located in the skin (melanocytes).
Scientists rightly wanted a molecule that treated chronic inflammation – and only inflammation – without having other unwanted effects.
The good news is KPV was determined to be the “minimum effective sequence” needed for α-MSH to exert its inflammation-lowering properties.
This was discovered as early as 1984 when a rabbit study demonstrated KPV’s ability to lower fever:
“The idea that the 11-13 amino acid sequence is important to the effect of the parent molecule was tested by giving lysine-proline-valine both centrally and peripherally to rabbits made febrile by IV administration of leukocytic pyrogen. The tripeptide reduced fever after both central (0.5-2.0 mg) and peripheral (2-200 mg) administration.
It appears that the 11-13 sequence is part of the message sequence of alpha-MSH with regard to antipyretic activity. However, the lower potency relative to that of the parent molecule suggests that other portions of the molecule are essential to full expression of the antipyretic effect.”
Many more studies later, KPV was concluded to “exert a similar or even more pronounced anti‐inflammatory activity as full‐length α‐MSH” (Source).
And given the absence of melanocyte stimulation (i.e. skin pigmentation effects), researchers believed they finally found what they were looking for.
How Does KPV Work?
Even though KPV is the active part of the a-MSH molecule responsible for its anti-inflammatory activity, KPV and a-MSH target inflammation via similar yet separate mechanisms:
“In vitro, macrophage activation, determined as release of [the chemokine KC] and interleukin (IL)-1β was inhibited by α-MSH and MTII [Melanotan II] but not by KPV.
Furthermore, macrophage activation by MTII led to an increase in cAMP accumulation, which was attenuated by SHU9119, whereas KPV failed to increase cAMP. The anti-inflammatory properties of KPV were also evident in IL-1β-induced peritonitis inflammation and in mice with a nonfunctional MC1-R (recessive yellow e/e mice).
In conclusion, these data highlight that the C-terminal MSH peptide KPV exhibits an anti-inflammatory effect that is clearly different from that of the core MSH peptides. KPV is unlikely to mediate its effects through melanocortin receptors but is more likely to act through inhibition of IL-1β functions.“
What makes KPV particularly effective is that this process directly happens inside your cells:
“KPV exerts its anti-inflammatory function inside cells, where it inactivates inflammatory pathways. KPV enters the cell and interacts directly with inflammatory signalling molecules inside the cell. It enters the nucleus of the cell and, once there, can inhibit the interaction of inflammatory substances and molecules”
In order for KPV on its own to exert its inflammation-lowering effects, it relies on a transporter peptide known as PepT1:
“One of the normal transport functions of gut epithelial cells is the absorption of small peptides from the diet by peptide transport activity. This is mediated via the H+-coupled oligopeptide transporter (PepT1) which is located at the apical membrane of intestinal epithelial cells (IEC) and which cotransports peptides and H+”
“…Since expression of colonic hPepT1 is up-regulated in IBD [inflammatory bowel disease], its transport activity constitutes a potential new target for anti-inflammatory therapies. Furthermore, the importance of hPepT1 expression by immune cells during intestinal inflammation should be evaluated as it may be therapeutically advantageous to develop PepT1-mediated anti-inflammatory drugs”
Which leads scientists to the conclusion that KPV has three parts to its mode of action:
“i) KPV reduces the two most important intracellular signaling pathways in the pathogenesis of inflammatory bowel diseases: the NF-κB and MAPK cascade pathways as well as the subsequent synthesis of pro-inflammatory cytokines, ii) the anti-inflammatory effect of KPV is mediated through the transporter PepT1, and iii) oral delivery of KPV reduces the severity of DSS- and TNBS-induced colitis in mice.
These results indicate that targeting KPV transport into both epithelial and immune cells may reduce the overall level of pro-inflammatory cytokine production by mucosal and immune cells and therefore raise the use of KPV as an attractive therapeutic strategy against [inflammatory bowel disease]”
One thing people commonly get wrong about inflammation is believing they have to completely eliminate it.
WRONG!
We are addressing CHRONIC inflammation, which — grossly oversimplified — means there’s too much of it going on.
One paper I was able to retrieve summarizes what KPV does best:
“… the broad anti‐inflammatory effect will not result in strong immunosuppression as seen with the corticosteroids or systemic calcineurin inhibitors.
Accordingly, activation of NF‐κB as well as subsequent expression of pro‐inflammatory molecules is never fully suppressed, but mostly only reduced.
In the absence of inflammation or pro‐inflammatory stimuli such as LPS or IL1, the anti‐inflammatory and immunosuppressive potential of α‐MSH and its peptides was usually weak or absent. “
The key is to have a fully optimized level of inflammation in your body at all times, rather than too much or too little.
Benefits of KPV Peptide

KPV on its own doesn’t have too many published studies available — PubMed only shows 70 results between 1973 and 2021.
Much of what we know about this peptide comes mostly from in vivo studies, in vitro studies, animal studies, a few small human trials, 4-5 biohackers at most, and fewer peptide physicians.
Moreover, a lot of KPV’s health benefits are derived from what is known about its precursor α-MSH.
But that’s not going to stop me from being early on what will be another asset to my toolbox of fully optimized health.
Let’s discover how KPV can help you live a longer life free of unnecessary illness!
Anti-Inflammatory
Based on the mechanism of action you just saw, it should be clear how and why KPV addresses chronic inflammation and restores the body to a state of homeostasis.
We know this because of a 2008 systematic review where 37 animal studies compiled between 1981 and 2008 showcase the consistent anti-inflammatory effects of α-MSH.
(REMEMBER: KPV is the active part of α-MSH that is arguably responsible for a good majority of its ability to lower inflammation)
What’s really interesting is how the anti-inflammatory effects have an extremely broad spectrum.
Across 5 separate species (rabbit, mouse, rat, guinea pig, squirrel monkey), the following disease states were studied:
- Fever
- Systemic inflammation
- Brain inflammation
- Arthritis
- Ocular inflammation
- Contact dermatitis
- Fibrosis
- Allergic airway inflammation
- Acute pancreatitis
- Gastrointestinal inflammation
Not to mention protection against cytotoxicity, being protective of numerous organs, and much more.
Just to showcase how significant these effects are, let’s look at two of the studies examined in the review.
One is a 2007 paper investigating how KPV worked on murine models of inflammatory bowel disease:
“…treatment with KPV led to earlier recovery and significantly stronger regain of body weight. Histologically, inflammatory infiltrates were significantly reduced in KPV-treated mice, which was confirmed by the significant reduction of MPO activity in colonic tissue after KPV treatment.
Supporting these findings, KPV treatment of transfer colitis led to recovery, regain of body weight, and reduced inflammatory changes histologically. In MC1Re/e mice, KPV treatment rescued all animals in the treatment group from death during DSS colitis.”
Another 2011 study examined the use of the derivative KDPT (Lysine-d-Proline-Threonine) in treating intestinal inflammation in mice:
“KdPT-treated animals showed markedly reduced severity of inflammation in both colitis models. In colonic epithelial cells, KdPT increased proliferation, accelerated closure of wounds, and improved transepithelial electrical resistance after stimulation with interferon-γ/tumor necrosis factor-α. Moreover, treatment with KdPT also prevented the loss of tight junction protein expression and improved barrier function in vivo.
KdPT acted independently of IL-1 receptor type I in vivo and did not affect melanogenesis in vitro. KdPT is capable of attenuating the course of experimental colitis in different models and maintains epithelial cell function. Furthermore, KdPT does not induce pigmentation, emphasizing the potential of this small molecule for the future treatment of IBD.”
(Source)
(NOTE: KDPT is believed to have more potent anti-inflammatory effects than both KPV and the entire α-MSH peptide)
Notice how reducing inflammation was just ONE effect: Other outcomes observed include real results in the form of body weight regulation and the restoration of cellular function.
Like I’ve always preached for years: You fix systemic inflammation and a lot of other health problems just “fix” themselves or magically disappear.
Antimicrobial Properties
Although this specific use of KPV requires more research, we already see major effects on two pathogens: The bacteria Staphylococcus aureus and the fungal Candida albicans.
This effect has been well-established since 2000 when a landmark paper demonstrated this effect:
“alpha-MSH peptides significantly inhibited S. aureus colony formation and reversed the enhancing effect of urokinase on colony formation. Antimicrobial effects occurred over a broad range of concentrations including the physiological (picomolar) range. Small concentrations of alpha-MSH peptides likewise reduced viability and germ tube formation of the yeast C. albicans.”
“Reduced killing of pathogens is a detrimental consequence of therapy with anti-inflammatory drugs. Because α-MSH has potent anti-inflammatory effects we determined influences of α-MSH on C. albicans and S. aureus killing by human neutrophils. α-MSH peptides did not reduce killing but rather enhanced it, likely as a consequence of the direct antimicrobial activity.”
Even more interesting is how KPV isn’t even the MOST effective out of all the α-MSH derivatives to have naturally existed or been synthesized!
This was discovered two years later when pharmaceutical company Zengen found the right combination of amino acids to deliver the most potent pathogen-killing effect:
“In this structure-activity study, the team developed several compounds that have greater candidacidal activity than a-MSH and, in fact, one particular peptide (number 19) killed nearly 100 percent (99.7 percent) of Candida cells over repeated experiments”
“The power of this new a-MSH analogue against C. albicans appears to be significantly greater than any other known peptides, as it is super-potent, super-stable and super-durable…We’ve not only improved upon Mother Nature by developing a ‘super’ peptide that kills C. albicans, but also may have unlocked the key to understanding how a-MSH really works – through a receptor in yeast which is yet to be identified.”
Considering how fungal infections are known to quickly develop resistance against existing treatments, it’s possible that we are already close to eradicating a multi-decade problem in the medical industry.
Improves Overall Gut Health
There’s a reason why your gut is commonly referred to as the “second brain” of your body: It quite literally plays a pivotal role in regulating every other organ in your physical vessel.
Whether it’s your brain, your heart, or your belly fat, your gut bacteria can play a major role in the development of age-related diseases.
As early as 1997, we already saw how a-MSH is vital for treating a common gut disorder known as inflammatory bowel disease (IBD):
“The peptide treatment had marked salutary effects: it reduced the appearance of fecal blood by over 80%, inhibited weight loss, and prevented disintegration of the general condition of the animals.
Mice given alpha-MSH showed markedly lower production of TNF alpha by tissues of the lower colon stimulated with concanavalin A; the inhibitory effect of alpha-MSH on production of inflammatory nitric oxide by lower bowel tissue was even greater.
The combined results indicate that alpha-MSH modulates experimental IBD, perhaps by inhibiting production within the gut of the local proinflammatory agents TNF alpha and nitric oxide, or by inhibiting inflammatory processes closely linked to these mediators.”
Sadly, the only study I could find directly using KPV involved treating a specific type of IBD called ulcerative colitis.
Just a brief overview of what the disease is:
“[It] occurs when the lining of your large intestine (also called the colon), rectum, or both becomes inflamed.
This inflammation produces tiny sores called ulcers on the lining of your colon. It usually begins in the rectum and spreads upward. It can involve your entire colon.
The inflammation causes your bowel to move its contents rapidly and empty frequently. As cells on the surface of the lining of your bowel die, ulcers form. The ulcers may cause bleeding and discharge of mucus and pus”
Back to the singular study… KPV was administered to mice via a special formulation of nanoparticles and the results were promising:
“These NPs successfully mediated the targeted delivery of KPV to key UC therapy-related cells (colonic epithelial cells and macrophages). In addition, these KPV-loaded NPs appear to be nontoxic and biocompatible with intestinal cells.
Intriguingly, we found that HA-KPV-NPs exert combined effects against UC by both accelerating mucosal healing and alleviating inflammation.
Oral administration of HA-KPV NPs encapsulated in a hydrogel (chitosan/alginate) exhibited a much stronger capacity to prevent mucosa damage and downregulate TNF-a, thus they showed a much better therapeutic efficacy against UC in a mouse model, compared with a KPV-NP/hydrogel system”
The majority of the remaining studies examining IBD and its conditions involved the derivative KDPT, which nevertheless goes to show how powerful KPV can be despite being only 3 amino acids long.
As a matter of fact, we have TWO human studies where KDPT directly resulted in a beneficial effect on ulcerative colitis without compromising on safety:
“Compared with placebo, K(D)PT (pooled group) resulted in significantly higher proportions of patients in remission at 2 and 4 weeks, (2 wk: P = 0.0349; 4 wk: P = 0.0278) and a significantly higher proportion of patients with CAI response at week 8 (P = 0.0434). K(D)PT (pooled group) met the primary endpoint after additional analyses. Because of high placebo response rates, subgroup analyses tried to identify patients with unquestionably active and more severe, but still moderate, disease (CAI score ≥9 or taking more than one concomitant medication). These subgroups showed earlier and statistically significant CAI responses to K(D)PT versus placebo. All doses of K(D)PT were well tolerated.” (Source)
“At Week 2 and Week 4, remission rates were approximately twice as high for pooled KdPT compared to placebo (2 weeks: p=0.0361; 4 weeks: p=0.0178). For 20 mg KdPT remission occurred earlier compared to 50 mg or 100 mg K(D)PT. CAI response rates lost significance at later time points due to unexpected high placebo rates from week 6 on. Patients with active and more severe disease (CAI ≥9 ; baseline medication : aminosalicylates + corticosteroids and/ or azathioprine) showed earlier and more pronounced response to KdPT compared to placebo (p=0.0156). KdPT was safe and tolerated well at the investigated doses with no difference between placebo and KdPT group” (Source)
Since the patients suffering moderately or severely saw the best response with respect to disease remission and alleviation of symptoms, it’s clear that KPV and its derivatives work in the real world.
And if you don’t believe me, we already have two peptide physicians who are seeing success with KPV treatment!
Dr. Neil Paulvin claims his patients have treated gut issues such as Crohn’s disease in 3 months when treated with KPV.
Dr. Linda Hayes has used KPV to help people who are suffering from chronic mold issues and persistent diarrhea.
Seems like KPV and BPC-157 are the two leaders when it comes to the use of peptides for enhancing overall gut health (likely via the reduced production of pro-inflammatory compounds).
Shows Promise In Treating Skin Conditions Such As Psoriasis
What of KPV could accelerate the healing of wounds and injuries, especially those inflicted on the skin?
Luckily, a-MSH’s anti-inflammatory effects are also observed in the skin for multiple disease states:
“α-MSH was shown to elicit a plethora of anti-inflammatory and/or immunomodulatory effects in a variety of animal models including experimentally induced cutaneous vasculitis, experimental psoriasis, experimental autoimmune encephalitis, allergic contact dermatitis, allergic bronchiolitis and colitis”
“..resolution of inflammation is further crucial to prevent the development of a chronic inflammatory process that finally may lead to hypertrophic scar and keloid formation (v. i.). Such chronic skin wounds are characterized by a proinflammatory phenotype, that is presence of macrophage infiltration, TNF immunoreactivity and neutrophil infiltration”
The really fascinating part, however, is the additional mechanism of angiogenesis (i.e. new blood vessel formation) that takes place:
“The increased vascularization and the angiogenesis that accompany chronic inflammation prolong and intensify the inflammatory response, which has researchers intrigued. It is believed that angiogenesis sustains inflammation by delivering oxygen and nutrients to support the increased metabolic needs of cells at sites of inflammation”
Sadly, the closest thing we have to a KPV study is an experiment done in human skin models where KDPT was shown to be effective at lowering skin inflammation induced by psoriasis:
“Psoriasis is a chronic inflammatory disease appearing as scaly erythematous cutaneous lesions, which are characterized by parakeratosis and acanthosis as well as the infiltration of immune cells, such as T helper-1 and T helper-17 cells”
“…systemic KdPT treatment significantly reduced hyperkeratosis and acanthosis in murine as well as human skin. Moreover, KdPT upregulated Foxp3 in CD4+ T cells from mice and from peripheral blood of individuals with psoriasis and decreased the expression of type 1 inflammatory cytokines, indicating that the beneficial effect of KdPT was, at least in part, mediated by the induction of functional regulatory T cells that suppressed the activation of pathogenic CD4+IFN-γ+ and CD4+IL-17+ T cells.”
Don’t despair… we do have two patents from Zengen for the use of KPV in treating dermatological disorders and treating skin cosmetically:
“According to the invention, the KPV peptide can also be used to prepare a composition intended to attenuate, or even make disappear, bedsores, caused in particular by prolonged bed rest. The invention also relates to the use of a peptide containing the tripeptide KPV, for the preparation of a composition intended to attenuate, or even to make disappear, blisters, cracks or crevices, or even after-effects of dermabrasions or of peeling, whether cosmetic or surgical, on the lips, hands, face or body.” (Source)
“It follows that the use of a preparation that could offer all the benefits of steroid preparations, antipyretics, analgesics, and antihistamines but without the attendant side effects, will be a great addition to the available avenues of treatment of these types of symptoms and these types of disorders… The present invention is directed to a treatment for dermatological disorders and a method for preventing dermatological disorders and their associated symptomatology… The [KPV] polypeptides are at a level to effectively treat the cutaneous inflammation, edema, erythema, opportunistic infection and pruritis, and are dissolved into a carrier.” (Source)
Who knows… maybe you’ll see KPV or one of its analogs in an Aseir Custom product someday. 😉
Other Therapeutic Applications
Seeing as KPV treats inflammation throughout the entire human body, its applications towards treating other disease states are great in number:
- Could be a potential therapeutic agent for treating immune hair disorders (i.e. hair loss due to an autoimmune disorder)
- Demonstrates “anti-HIV properties in infected cells”, as evidenced in a cell culture study
- KdPT, a very similar analog to KPV, may be useful in treating acne while α-MSH shows promise in addressing eczema
- Low levels of α-MSH are observed in conditions such as Lyme disease and mold illness, along with arthritis
- α-MSH plays a pivotal role in regulating ocular immunity, which is why it’s being investigated in an ongoing clinical trial
- In a mouse study, KPV lowered inflammation and tumorigenesis during colitis-associated cancer
- α-MSH has implications in treating disorders like “asthma, sarcoidosis, and the acute respiratory distress syndrome” (Source)
The faster we get more clinical research in humans, the better off humanity will be.
KPV Peptide Dosage

Unlike other therapeutic peptides that tend to exist solely in one formulation, KPV can be administered in 3 different ways.
According to chiropractor Jason Pencek, owner of the wellness clinic NutrIV Therapies, the recommended KPV dose depends on how you choose to take it.
Oral (via tablet)
- Two 250 mg capsules taken with or without food, until your ailment is healed
- Doses can be as high as 2000 mg per day depending on the condition being treated
- Best used for treating Crohn’s disease, ulcerative colitis, and irritable bowel syndrome (i.e. gut problems)
Subcutaneous Injection
- 200-500 mcg injected once a day
- Best used for treating overall systemic inflammation
Topical Cream
- 7.5 mg applied to the affected area twice a day (Source)
- Best used for treating psoriasis and cystic acne
I consulted with BioLongevity Labs, and their advised dose of KPV for each formulation was identical.
Due to KPV’s non-existent data in human subjects, you should allow yourself 3-4 weeks before any significant changes take place.
I also recommend keeping this peptide at room temperature and away from bright light and humidity.
KPV Side Effects and Safety

Some reported side effects of KPV from humans who have used the peptide in the past include:
- Brain fog via an apparent sedative effect
- An “orange” stain left on the skin after topical application that washes off in a few days (distinct from increased skin tanning)
- A possible local skin reaction from topical application
It is also suggested you do not use KPV if you are nursing, may become pregnant, or are already pregnant.
Aside from these minor and rare occurrences, the currently available data suggest KPV has an excellent profile.
To start, we already have studies done in vivo, in vitro without any unwanted side effects, and in mice demonstrating therapeutic efficacy without any unwanted adverse events.
And this appears to be true regardless of how KPV was administered.
We also know the more potent analogs of α-MSH are safe even when used at extremely high doses:
“In terms of the safety profiles of α-MSH and its tripeptides, very few data are currently available due to lack of toxicity studies. However, the super-potent analog of α-MSH, [Nle4-D-Phe7]-MSH, when administrated intravenously at doses of up to 0.6 mg/kg, results in occasional gastrointestinal upset and facial flushing without major detrimental effects.
In this scenario, α-MSH and its tripeptides should have better safety profiles compared to traditional immunosuppressive therapies and biologics, known to cause liver and kidney injury, bone marrow suppression, gastrointestinal upset, hypertension, and dyslipidemia.”
“…compared to α-MSH, KPV, and KdPT might confer more advantages to be utilized as clinical therapy for the treatment of immune-mediated inflammatory disorders since they are easier to synthesize due to smaller size and lower cost, theoretically with no pigmentary effect, more resistant to bacterial infection, and more easily to be administrated locally for several inflammatory diseases”
And even though α-MSH’s precursor ACTH (Adrenocorticotropic Hormone) can significantly reduce fever in rabbits, it appears as if α-MSH does not come with ACTH’s side effects:
“Studies comparing the antipyretic activity of centrally-administered alpha MSH to the widely-used antipyretic, acetaminophen indicate that alpha MSH is much more potent in reducing fever than acetaminophen, and that alpha MSH was more than 2500 times more potent by weight than acetaminophen in reducing fever”
“ACTH was used to reduce clinical and experimental fever soon after it was first described, but this peptide also stimulates corticosteroid release, and can, with repeated administration, result in Cushing’s syndrome. On the other hand, the shorter alpha MSH molecule, which is derived from ACTH, does not stimulate steroid release and there appears to be no irreversible deleterious effects when given to rabbits or to man.”
So due to the non-steroidal nature of KPV and its precursor α-MSH, the peptide can be used for as long as needed until the indicated ailment is healed.
However, there are some problems with the small size of KPV that may not make it the best analog for treating inflammation:
“The use of this peptide as an anti-inflammatory agent is limited by its low selectivity between the different melanocortin receptors, susceptibility to proteolytic degradation, and rapid clearance from circulation.
Even though α-MSH has some effects as a successful anti-inflammatory agent, its use as a systemic therapeutic agent is not appealing because of undesirable effects on hormonal regulation.”
So the goal for researchers right now is to fix “proteolytic instability, immunogenicity, low oral bioavailability, and short half-life” while also improving “the target specificity, membrane permeation, stability, solubility, and oral bioavailability of the drug without altering the therapeutic activity” (Source).
The good news is that efforts to do so are already well underway:
- Using analogs such as KdPT and (CKPV)2 that have better anti-inflammatory and anti-fungal activity
- Administering KPV through different drug delivery vehicles such as nanoparticles and iontophoresis
(CKPV)2 is the most interesting as it’s literally two units of KPV attached to each other:
“The synthetic peptide (CKPV)2, also named CZEN-002, was designed based on the KPV (α-MSH11-13) peptide. The peptide is a dimeric octamer peptide comprising two units of KPV peptide connected by a cysteine-cysteine linker, which is classified as loop peptide. The (CKPV)2 peptide revealed outstanding candidacidal activity against C. krusei and C. glabrata that are emerging as drug-resistant strains, but it showed very low toxicity to host cells”
CZEN-002 belongs to pharmaceutical company Zengen Inc., which is currently pending Phase II trials to use it as an intravaginal gel for the treatment of vulvovaginal candidiasis (i.e. a vaginal yeast infection).
However, since the trials were planned all the way back in 2005, it’s unlikely we’ll see it as an FDA-approved drug anytime soon.
Where to Buy KPV
Due to KPV being a brand new contender to the therapeutics peptide space, very few vendors stock it (let alone have any awareness it even exists).
But there’s only one source you should be using to get your hands on it: BioLongevity Labs
Use code JAYC to get 15% off your order!
They are the only peptides company I would endorse and trust to safely and effectively provide KPV at the highest quality and purity possible.
Keep in mind this is the formulation used for subcutaneous injections, so use it appropriately.
Additional Reading Resources For KPV

There isn’t a whole lot I can offer in terms of extra information about KPV — the lack of human studies leaves high-consciousness biohackers like myself and others wanting more research to be done.
But until that day comes along, here are some recommended articles to dig further into this peptide…
Functional medicine internist Dr. Kim Crawford talks about novel therapies to treat Crohn’s disease and ulcerative colitis, including other peptides such as GHK-Cu and BPC-157.
The Medicine With Heart Institute has a great 6-minute video summary discussing all of the main points in this article.
The Genemedics Institute has compiled 97 studies about KPV and many of its other possible benefits (based on being derived from α-MSH) that include protecting against stroke and nerve damage.
And as always…
Raise Your Vibration To Optimize Your Love Creation!
PS – When you’re ready to learn how to use peptides at a much deeper level, you have two options.
- You can set up a private One on One Call with me.
- Joining The Fully Optimized Health Mastermind with two Monthly 60 Minute Group Coaching Calls with Me and Daniel Kelly Discussing Fully Optimized Living including Peptides, Hormones, Gray Market Agents, Performance Enhancement and Raising Your Vibration.


