 Written by Jay Campbell
Written by Jay Campbell


Human Growth Hormone (hGH) has been a vital element of every bodybuilder’s toolbox since the late-20th century — one of the magical items that seemingly doesn’t get mentioned alongside the phrase “eat clean and train hard”
But perhaps there’s a new way to use it… or new compounds that confer similar if not greater positive biological effects we want without mythical side effects.
What advancements in science have we made to truly understand what human growth hormone can and can’t do?
And what strategies exist to optimize our body’s own natural production of growth hormone 24/7?
NOTE: This article will heavily borrow from the pieces I have written about Ipamorelin, Tesamorelin, and CJC-1295 in order to create a comprehensive overview of hGH.
Doing so ensures you will understand how hGH and all its related compounds are both similar and different.
What is Human Growth Hormone (hGH)?

The name is self-explanatory – HGH is literally responsible for bodily growth from the moment you are born:
“Human growth hormone (hGH) plays a vital role in growth and development. It is naturally produced by somatotropic cells in the anterior pituitary gland. The hormone is produced as a 217 amino acid precursor protein. The 26 N-terminal amino acids correspond to a signal peptide, which is essential for hormone secretion. This signal peptide is cleaved during the secretion process to yield the mature, 191 amino acid form of hGH.”
“…hGH is produced in the anterior pituitary gland and is circulated throughout the body. hGH interacts with a variety of cells while in the bloodstream including muscle and bone cells. It eventually reaches and stimulates growth of all major organs (particularly the liver where it stimulates the production of growth factors) with the exception of the brain”
The mature form of hGH is also known as somatotropin, and its production is heavily regulated by numerous compounds:
“Growth hormone-releasing hormone (GHRH), produced in the hypothalamus… functions to promote hGH production and release. hGH will [also] negatively feedback into the hypothalamus, thus decreasing GHRH production.
“Somatostatin, produced in various tissues throughout the body… inhibits the release of GHRH as well as the hGH release response to GHRH stimulus and increases in hypoglycemia”
“Ghrelin, produced in the gastrointestinal tract as part of the hunger response… is [functionally] protective against hypoglycemia. When elevated, ghrelin binds to somatotrophs to stimulate hGH secretion.
“Insulin-like growth factor-1 also acts to inhibit hGH by both directly inhibiting somatotrophic hGH release and indirectly through synergistically increasing the release of somatostatin.”
With regards to hGH’s mechanism of action, it’s quite complicated to explain.
Given its discovery as a literal “hormone of growth” in the early 1910s and the recognition of its multi-fold importance in numerous biological systems 50 years later… there are quite a few academic textbooks dedicated to this question alone.
But just to give you the Cliff Notes summary, here’s what you need to know:
“hGH increases the uptake and incorporation of amino acids into muscle.
hGH has acute, transient insulin-like effects that stimulate glucose uptake into muscle and adipose tissue.
However, its chronic effects are antagonistic of insulin, leading to fatty acid mobilization, inhibition of glucose uptake, and reduced insulin sensitivity.
hGH also has indirect effects mediated primarily by insulin-like growth factor-1 (IGF-1), although its mechanism of action is poorly understood.“
The two YouTube videos below are useful for the endocrinology nerds who want to dig even deeper into hGH’s downstream effects in the human body:
Human Growth Hormone Benefits

If you read the pieces mentioned at the start of this article, you have already seen hGH’s numerous health benefits and the scientific evidence to back up all the claims made.
Yet for the sake of brevity, here’s a friendly reminder:
“hGH, produced by the pituitary gland, spurs growth in children and adolescents.
It also helps to regulate body composition, body fluids, muscle and bone growth, sugar and fat metabolism, and possibly heart function.
Produced synthetically, hGH is the active ingredient in a number of prescription drugs and in other products available widely over the Internet.”
Incredibly, the most common uses for hGH are not FDA-approved.
Some people use the hormone, along with other performance-enhancing drugs such as anabolic steroids in an attempt to build muscle and improve athletic performance.
Yet hGH’s effect on athletic performance is unknown at least in the world of science aka peer review.
Because Human Growth Hormone levels naturally decrease with age, some so-called anti-aging experts have speculated hGH products could reverse age-related bodily deterioration.
But these claims, while interesting, are unproven.
The use of HGH for anti-aging is not FDA-approved.”
(Ignore the bureaucratic nonsense about “FDA approval” — you’ll quickly see why it’s bunk as you continue reading)
But the quote does get one thing right: The body’s natural decrease of hGH production over time (~1-2% lower every year after age 30), especially after puberty is done, has led many biohackers down a path of wanting to continuously stimulate hGH production as on ages.
Funnily enough, hGH’s relationship with improved body composition can be regarded as a “chicken and egg” problem:
“Studies carried out in the late 90s have uniformly documented that adults with severe GH deficiency are characterized by increased fat mass and reduced lean body mass (LBM).
It is also known that normal GH levels can be restored in obese subjects following massive weight loss, and that GH substitution in GH-deficient adults normalizes body composition.
What remains unknown is the cause-effect relationship between decreased GH levels and senescent changes in body composition.
Is the propensity for gaining fat and losing lean mass initiated or preceded by a primary age-dependent decline in GH secretion and action?“
Another thing worth mentioning is that there ARE FDA-approved conditions for which hGH is used as a treatment, all of which stem from a lack of hGH production:
“GH deficiency is one of the many causes of short stature and dwarfism.
It results primarily from damage to the hypothalamus or to the pituitary gland during fetal development (congenital GH deficiency) or following birth (acquired GH deficiency).
GH deficiency may also be caused by mutations in genes that regulate its synthesis and secretion
… In some cases, GH deficiency is the result of GHRH deficiency, in which case GH secretion may be stimulated by infusion of GHRH.
In other cases, the somatotrophs themselves are incapable of producing GH, or the hormone itself is structurally abnormal and has little growth-promoting activity”
A quick look at the product monograph for somatotropin (i.e. hGH) reveals the conditions in question, which are extremely rare in nature:
“Somatotropin is indicated for the treatment of pediatric patients who have growth failure due to an inadequate secretion of endogenous growth hormone, short stature associated with Turner syndrome, Prader-Willi syndrome (PWS), idiopathic short stature (ISS), short stature or growth failure in short stature homeobox-containing gene (SHOX) deficiency, and short stature born small for gestational age (SGA).
It is also indicated for adults with adult-onset growth hormone deficiency, either alone or associated with multiple hormone deficiencies (hypopituitarism), as a result of pituitary disease, hypothalamic disease, surgery, radiation therapy, or trauma.
It is also used to treat childhood-onset growth hormone deficiency in adults due to congenital, genetic, acquired, or idiopathic causes”
In other words — you ALREADY KNOW if you have any of the problems listed above.
I’m reminded of this humorous story from a dating coach who didn’t consistently use hGH shots prescribed to him at age 13, and now has to take full ownership for being short in his adult life:
“…however bad you feel about the physical traits you were born with, I almost guarantee I’ve felt worse.
I’m the reason I’m short.
At the age of thirteen, I was diagnosed with growth hormone deficiency. My body wasn’t producing enough and I needed shots to grow normally.
By sixteen, I stopped taking the shots as often as instructed.
They hurt and interfered with hanging out with friends. I was young, naive, and didn’t realize the impact it would have.
I could have been about 5’10”.
This might not seem like much but it’s the difference between being average or above average versus being short.
Once I became an adult, the realization was devastating and I hated myself because of it for a long time”
If only the poor bastard had understood the benefits of insulin syringes.
Scientific Truth vs. Bro-Science Myths: Separating the Reality of Human Growth Hormone From Fiction

Before we get into the meat and potatoes of maximizing hGH production no matter your age, there are a few myths we have to put aside…
MYTH: hGH will get you the perfect physique without having to leave your couch.
FACT: hGH will only work for people who have spent many years striving to reach their maximum physical (musculature) potential (through focused training) dictated by a combination of their genetics, and more importantly, their ‘epigenetics’.
MYTH: Since hGH is naturally produced by the human body, there shouldn’t be any side effects associated with exogenous use.
FACT: hGH, like every other hormone in your body, exists at an OPTIMIZED level.
The trick is to find what that “level” is for YOUR body and then strive to keep it there.
If supplementing with hGH in too high of dosages, there is a biological limit one may surpass that can produce a disease condition known as “acromegaly”:
“Acromegaly is a rare hormonal condition that results from an excess amount of growth hormone (GH) in the body.
The extra amount of GH causes excess growth in the bones and soft tissues of the body. This disease is often seen in children leading them to grow to abnormal heights.
They may also have an exaggerated bone structure as acromegaly normally affects the arms, legs, and face”
“Common symptoms include enlarged bones in the face/feet/hands, excessive growth spurts, swollen and painful joints that limit movement…, spaces between the teeth, splayed fingers and toes, fatigue, headaches, an inability to sleep, muscle weakness, profuse sweating, thickened skin”
And even if you don’t reach that point, there are real side effects of hGH injections when used in excess:
“Possible side effects include: muscle aches, joint discomfort, headaches, swelling of the hands and feet… hGH can affect insulin usage in the body, so people with diabetes should monitor their blood sugar levels carefully.
If the levels of hGH are too high in adults, they may experience: muscle or joint pain, fluid retention, carpal tunnel syndrome.
There is also a risk of excess hGH dosing speeding the rate of tumor formation if one was genetically predisposed to some form of cancer. (This is now a hotly debated topic in the field of endocrinology and more science in health aging adults is necessary. Most of the studies where cancer shows up is with people already co-morbid or suffering from acromegaly.)
Adults cannot grow taller by using growth hormone.
Higher doses will thicken the person’s bones instead of lengthening them.
The skin area can also be affected and may turn thick, coarse, and hairy.
Excess hGH levels can also lead to high blood pressure and heart disease.”
MYTH: hGH use will dramatically increase my performance in the gym by helping me push more weight.
FACT: hGH may improve your physical appearance, but don’t bet on sprinting faster or increasing your 1-rep max (Jay’s Comment: unless it’s combined with Testosterone and or Insulin.
This may seem a bit paradoxical, so stick with me.
As an old article from Slate correctly notes, muscle appearance DOES NOT directly translate to improved athletic performance:
“A chiseled physique won’t help you hit a baseball or throw a punch.
So far, no one has been able to connect the increase in lean body tissue caused by HGH with enhancement of athletic performance. (Jay’s comment: Although continual practice and skill acquisition in combination with GH/Testosterone/Insulin would ‘likely’ find the connection).
Unlike anabolic steroids, growth hormone (in isolation) hasn’t been shown to increase weight-lifting ability; (Jay’s comment: in the lab, it has a greater effect on muscle definition (making the muscles more pronounced ie dense due to GH burning the visceral and subcutaneous fat around them) than muscle strength“
This is backed up by an older systematic review which showed that strength gains are only measurable and mostly attributable to hGH in people who are ALREADY deficient in hGH.
The article from Slate expands on why athletes continue to take hGH — and hence why HGH continues to be a banned doping substance:
“One possibility is that the drug really does enhance performance but that the effect is too subtle to measure in a controlled setting.
(Jay’s comments: Remember, no study is able to be replicated due to human bio-individuality. We are all n-of-1.)
An elite athlete might be able to detect very slight improvements in strength and agility that would be invisible to lab scientists or statistical tests.
At the highest levels of sport, a tiny edge can make a big difference.
Athletes might also derive some added benefit by mixing hGH with other drugs (Jay’s comments: Insulin and Testosterone are the known culprits in the professional body building ranks).”
“…The World Anti-Doping Agency will ban any drug that athletes use, whether or not it has an effect.
The WADA code points out that the use of substances ‘based on the mistaken belief they enhance performance is clearly contradictory to the spirit of sport.’
In other words, it doesn’t matter if hGH gives athletes an unfair advantage.
If Jerry Hairston believes he’s cheating, then he really is cheating.” (Jay’s comments: This is obviously ridiculous to anyone that has used hGH in combination with Testosterone whether therapeutically or supra-physiologically. The real world benefits are obvious and noticeable (from a performance and aesthetic measurement).
This is something worth thinking twice about for the younger readers who are competing in sports or performance athletics.
Obviously, as evidenced by the cartoonish aesthetics exhibited by professional body builders from the last 30 years, supra-physiologic dosages of hGH in combination with Anabolic Steroids and Insulin clearly provide an added benefit to building muscle and reducing body fat.
MYTH: hGH use will increase lifespan and reverse 2 decades’ worth of aging.
FACT: hGH is not proven to be a direct anti-aging agent, but its health benefits can DEFINITELY help you better engage in already-proven anti-aging activities.
This information comes from a study published 31 years ago and the flaws are obvious to even a non-scientist:
“Twelve healthy men, 61 to 81 years of age, who had serum concentrations of insulin-like growth factor I below those found in normal young men received growth hormone for six months.
The weekly dose of growth hormone was approximately twice as high as the dose used in adult men with a growth hormone deficiency.”
“The administration of growth hormone in older men resulted in a 4.7-kg increase in lean body mass, a 3.5-kg decrease in adipose mass, and an increase of 0.02 g per square centimeter in lumbar-spine density; systolic blood pressure and the fasting glucose concentration increased significantly.
The study was not double-blind (there was a control group consisting of nine men who received no treatment); there were no assessments of muscle strength, exercise endurance, or quality of life”
Unfortunately, this one paper was the basis for the SCAM products and advertisements claiming to take years off your age with oral and topical hGH formulations that do diddly squat.
You know the kind sold in every health food, supplement store and multi level marketer on planet earth from 2010 thru 2019.
But that’s only in discussing worthless supplements, gels and secretagogues found over the counter everywhere.
What about using real pharma grade hGH like Genotropin from Phizer or Norditropin from Novo Nordisk?
What would the results of a clinically precise dosage administered for 15-30 years in an aging Man or Woman who was also already living a fully optimized lifestyle provide?
I would venture to say a whole hell of a lot from a stand point of maintaining vitality, well being, sexual function and low body fat (the most tried and true method of avoiding inflammation as one ages).
Unfortunately there are no studies for the use of pharmaceutical grade hGH in clinical dose fashion to combat aging in otherwise healthy people over time.
From feedback from highly intelligent and sophisticated people using hGH in such a precise fashion as they age (I might know ‘a few’ of these folks), the reviews are pretty stunning.
“Life altering”,
“Wellbeing is unlike anything else”,
“I maintain low body fat year round with minimal dietary intervention”,
“Therapeutic Testosterone in combination with 2 iu’s of pharma grade hGH Mon thru Friday is the Elixir of the Gods”
hGH and Peptides Differences

With an understanding of hGH, let’s dive into why aging men and women might focus on using peptides instead of hGH.
- Increased risk of insulin resistance with prolonged use (Jay’s Comments: this would be completely minimized if not eliminated altogether by using Metformin or Dihydroberberine concomitantly)
- Natural hGH production may be reduced and or shut down with continuous high dosage hGH injections (Jay’s Comment: There is no real proof of this especially if used in a small clinical dose first thing in the morning on an empty stomach in order to not disturb normal nightly sleep cycles)
- Pituitary function may be negatively affected (Jay’s Comment: I would agree but only if the dosage was too high and for too long without any cessation or break from usage)
- An increased risk of tachyphylaxis in higher dosages (Jay’s Comment: The difference between an effective adjuvant and a poison is always the dosage administered)
- Costs at least $25,000+ per year (in the USA) when using the highest quality pharmaceutical hGH (Jay’s Comment: Sadly this number greatly prevents the majority of humanity from ever using pharma grade hGH)
- Hard to obtain as hGH is a CONTROLLED substance in many countries and noticeably counterfeited by the Chinese (Jay’s Comment: This is the primary reason in my estimation to avoid using hGH. One must be absolutely certain of their source)
Because of all those reasons, peptide physicians and biohackers have found a viable solution-Therapeutic Peptides.
The trick to maintaining the body’s natural production and release of growth hormone is to stimulate the PATHWAYS associated with growth hormone synthesis and distribution, rather than”forcing” more of it into the body as is with injecting hGH.
And this is where we get into two separate classes of biomolecules created to achieve this very purpose…
Growth Hormone-Releasing Hormones (GHRHs)
As discussed at the beginning of this article, GHRHs stimulate your brain’s pituitary gland to increase the production and secretion of hGH.
But you can’t just inject the 44-amino-acid GHRH itself into the body as it is rapidly degraded by your body’s enzymes and quickly becomes biologically inactive.
So in order to overcome this issue, synthetic analogs of GHRH had to be created:
 (Source)
(Source)
There are a number of them in existence, so let’s go over them one by one…
Sermorelin (a.k.a. GRF [Growth hormone Releasing Factor] 1-29) consists of amino acids #1-29 of the original GHRH molecule, the active region responsible for stimulating the pituitary gland to produce HGH. For this reason it is also used as a tool for “diagnostic evaluation of pituitary function” (Source).
And even this was enough to confer “physiological and clinical advantages” over hGH:
“Unlike exogenous recombinant hGH that causes production of the bioactive hormone IGF-1 from the liver, sermorelin stimulates the patient’s own pituitary gland by binding to specific receptors to increase production and secretion of endogenous hGH.
…Effects are regulated by negative feedback involving the inhibitory neurohormone, somatostatin, so that unlike administration of exogenous rhGH, overdoses of endogenous hGH are difficult if not impossible to achieve,
…Because of the interactive effects of sermorelin and somatostain, release of hGH by the pituitary is episodic or intermittent rather than constant as with injected recombinant hGH.
…Tachphylaxis is avoided because sermorelin-induced release of pituitary hGH is not “square wave”, but instead simulates more normal physiology”
Unfortunately, at a half-life of 5-10 minutes, it is metabolically cleared just as fast as its predecessor via rapid enzymatic cleavage of the amino acids.
Mod GRF 1-29 (a.k.a. Modified GRF 1-29, or “CJC-1295 without DAC”) involved making changes to select amino acids within the Sermorelin molecule, as highlighted in yellow on the diagram (#2, #8, #15, and #27).
The end result is improved biological stability, higher binding affinity to GHRH receptors, and a longer half-life of 30 minutes.
CJC-1295 (a.k.a. “CJC-1295 with DAC”) adds on a “Drug Affinity Complex” (DAC) to one end of the Mod GRF 1-29.
This significantly extends the molecule’s half-life to 6-8 days, although Ben Greenfield believes “this extended half-life may not provide the optimal pulses of GH by the pituitary that we see as pulsatile when naturally occurring” (Source).
Tesamorelin is the only FDA-approved molecule on this list and takes a different approach to modify GHRH: Adding the trans-3-hexanoic acid at the start of the molecule was another way to increase metabolic stability and potency with respect to stimulating GH production.
As for what it’s approved for, it’s prescribed to treat the excessive buildup and abnormal distribution of visceral fat tissue in HIV patients (i.e. lipodystrophy).
And why I love this peptide for reducing body fat off the midsection aka belly area.
Growth Hormone-Releasing Peptides (GHRPs)
Dr. William Seeds, one of the most knowledgeable physicians for therapeutic peptides, brilliantly explains why GHRHs by themselves are not enough to stimulate the continuous release of hGH.
If your memory is sharp, you’ll remember the inhibitory role of somatostatin:
“The machinery in the anterior pituitary secretagogue is set in motion to produce the pulse of growth hormone, but the hypothalamus still controls the release of GH, with somatostatin having a rate-limiting effect.
In this way, though GH will eventually be released, it will not be until somatostatin inhibition is lifted.
For this reason it’s important to consider using a GHRP in combination to ensure endogenous GH release within a 20-minute window”
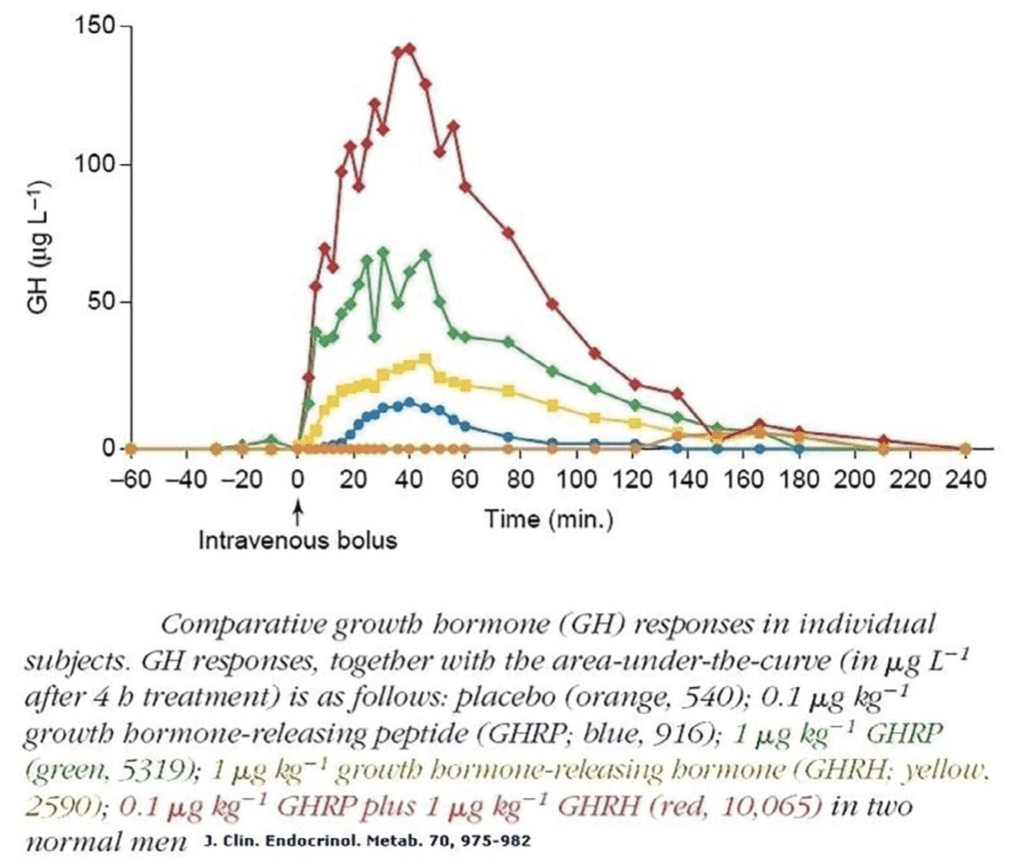
Or as Ben Greenfield says it best:
“In a nutshell, the main reason to use this a GHRH in conjunction with GHRP and GH is to cause an even greater increase in GH than you’d get if you used GH by itself, and also to minimize the negative side effects of using GH by itself.
Remember what you learned earlier: GHRP’s release a pulse of GH, and then the GHRH’s release and amplify this pulse.”
The GHRPs and GHRHs work synergistically to maximize the endogenous release of GH from the pituitary gland, as the resulting “pulse” is much greater than if the GHRH is used on its own.
So what GHRPs are available at our disposal?
At this time, Ipamorelin is the only one I can recommend as it SELECTIVELY stimulates the release of hGH without affecting luteinizing hormone (LH), follicle-stimulating hormone (FSH), or thyroid-stimulating hormone (TSH), prolactin, and cortisol.
Inadvertently elevating these bodily hormones can lead to unwanted side effects such as weakened immunity and elevated blood pressure.
The same selectivity is not observed in other GHRPs, which are not used for very obvious reasons according to Dr. William Seeds:
- Hexarelin: The strongest GHRP, known to give the biggest pulse of all — Desensitization happens at any dose
- GHRP2: 2nd strongest GHRP; desensitization is unclear when used beyond saturation dose.
- GHRP6: 3rd strongest GHRP; desensitization does not occur if shots are broken up.
- MK-0677: IGF-1 response may be supra-physiological
In my opinion, none of these GHRP’s are worth using due to their various negative side effect profiles.
Especially in comparison to the other peptides mentioned already.
So in short, we have two GHRH agents (Tesamorelin and CJC-1295) and one GHRP (Ipamorelin) agent we can rely on for maximizing natural HGH production without compromising bodily function when breaking from the injections of any of these peptide protocols.
hGH vs. Peptides: When is One Better Than the Other?
This is a tough call due to the lack of available research on using hGH in healthy and optimized aging men and women and the availability of pharmaceutical grade hGH ‘legally available’.
Let’s just say in most cases due to the limitations discussed in the previous sentence, the GHRPs and GHRHs (Ipamorelin, CJC-1295 and Tesamorelin specifically) are a better option to using hGH for ‘most people’.
I would quantify those thoughts with this statement.
If you are an aging man or women with resources, who lives in a country where Genotropin and or Norditropin is legally available, 1-3 iu’s per day (5 Days On, 2 Days Off), in combination with Hormone Optimization, Metformin, Dessicated Thyroid supplementation and an insulin controlled lifestyle (dietarily) would be the optimal choice.
I would choose this protocol over therapeutic peptides all day and twice on Sunday.
There is ONE issue rarely discussed on podcasts or articles found online about peptides vs hGH.
When does an aging person have to choose hGH over Peptides due to the lack of IGF-1 production in the body?
(IGF-1, also known as somatomedin-C, is a polypeptide hormone produced by the liver and other tissues in response to growth hormone release by the pituitary gland. IGF-1 mediates the action of growth hormone, and its concentration reflects the circulating concentration of growth hormone in one’s body. )
It is theorized that IGF-1 along with Testosterone never completely stops as one ages but just declines steadily.
Proving this assumption would be an entire article by itself because the only way to know would be to test for IGF-1 production yearly as one ages (starting at around 60).
This can be easily done by visiting any Private Lab Testing Company like Private MD Labs.
Somatopause is the scientific term for when an adult reaches a point of supremely low IGF-1 levels.
But is this really true (as theorized as a slow steady decline) knowing how contaminated our environment is due to modernization (EDC’s etc)?
It is my opinion there will come a time in a man or woman’s life, when only hGH will be an effective mediator against age related decline.
If you are an aging Man or Woman, I recommend getting your IGF-1 levels looked at starting at around 55 and once a year from then on to be certain of the limits of your natural production.
I do realize that IGF-1 is just one gauge of understanding growth hormone as one ages, but measuring it at a private lab annually won’t hurt your cause.
When (and How) to Use Human Growth Hormone
Who should be using hGH, what doses of hGH should you use, how old do you have to be to use hGH, and for what reasons would you use hGH?
When it comes to age, I would say at a minimum you should be an adult (40+) UNLESS your primary physician has you using hGH for an FDA-approved purpose.
And with regards to dosage timing, follow Dr. William Seeds’ advice regardless of what purpose you use hGH or its peptide analogues:
Avoid food consumption 30 minutes before use and 1.5 hours after use (due to carbs (insulin) and fats blunting hGH release).
From the life extension world, most aging men and women who regularly use hGH take it first thing in the morning upon arising, in order to not interfere with the body’s natural production of GH during the night time sleep cycle.
The Bottom line: Use hGH on an empty stomach or fasted in order to prevent circulating insulin (from food consumption) from minimizing the effects of its release and absorption.
When injected, the circulating half-life of hGH is relatively short (20-30 minutes), while its biological half-life is much longer (10+ hours) due to its indirect effect in biological system functioning.
Let’s get into the specific use cases for Human Growth Hormone!
Jay’s Comment: Fasted Cardio within 15-30 minutes of hGH administration in the morning is a nuclear weapon for torching stubborn visceral and or subcutaneous body fat in men and women due to the growth hormone targeting the stubborn fat tissue while helping to burn free fatty acids floating around in the blood stream.
hGH For Longevity and Body Composition Change
From the anti-aging and life extension communities around the world, ‘most people’ use the following dosages.
Men inject hGH into the subcutaneous fat around the navel at anywhere from 1.5-3 iu’s per day on a schedule of 5 days on and two days off.
Women inject hGH in the same way at anywhere from 1-2 iu’s per day with a similar dosing strategy.
Pro Bodybuilders and performance athletes often use much larger (higher) dosages(10 iu’s + per day and often in combination with Insulin).
It’s important to understand the advice I AM providing in this article is in the context of health and longevity only.
Peptides for Longevity and Body Composition Change
Although these GHRPs and GHRHs are theoretically decent at inducing anabolism (especially when combined with Therapeutic Testosterone), I’ve personally noticed they are far more effective as fat loss agents.
So here are my preferred peptide protocols, starting with my most recommended ones for fat loss (Men is slightly different from Women) and next for inducing anabolism/strength (provided the diet is dialed in to provide ample carbohydrates for refueling muscle glycogen stores).
Tesamorelin
- 1 mg injected subcutaneously at night before bed (but at least 90 minutes after your last meal), and 1 mg injected subcutaneously upon waking up in the morning (ideally before fasted cardio or exercising). (This is the blowtorch for eliminating lower abdominal and belly fat for men provided diet and exercise are also dialed in). 6-10 weeks of usage to ensure there is no anti-body formation or build up and to maximize the results.
Ipamorelin
- 100-300 mcg injected subcutaneously 1-3 times a day. (For women 200 mcg injected right before bed will provide amazing results in relation to improving skin elasticity, deeper sleep cycles, and altering body composition to more muscle and less body fat (assuming diet is dialed in). I recommend cycles of no longer than 8-10 weeks followed by an equal amount of time off.
Tesamorelin + Ipamorelin
- 100 mcg Ipamorelin in the morning and 1 mg of Tesamorelin + 100 mcg Ipamorein injected subcutaneously before bed
- Cycle within the week for 5 days on and 2 days off (i.e. use both peptides from Monday to Friday)
- Follow the weekly cycle for 6-8 weeks before taking an equal amount of time off. *WARNING* This peptide cycles will cause water retention but make one incredibly strong and energetic.
CJC-1295 without DAC + Ipamorelin
- 200 mcg Ipamorelin and 200 mcg CJC-1295 without DAC injected subcutaneously on a daily basis — 5 days on, 2 days off. This produces a pronounced fat burning effect similar to 1-2 iu’s of pharmaceutical hGH. 8-10 week cycles followed by an equal amount of time off.
Jay’s Comment: All of these GH inducing or releasing agents do cause subcutaneous water retention.
The amount of water one will hold depends on a number of factors, including diet, dehydration levels, select vitamin, mineral and electrolyte levels and last but not lease, the quality of your sleep cycle.
It is well known in the body building and performance enhancement arena’s that when using Peptides or hGH, the user must cycle off at least 10-14 days before the day of their event in order to drop all intra-cellular water from the physique.
This is done to present the ‘leanest, stage ready appearance’ of the competitor.
If you are a biohacker using these agents to get into the ‘your best shape possible’, for a photo shoot or a beach vacation, always take this into consideration.
Is Human Growth Hormone Legally Available?
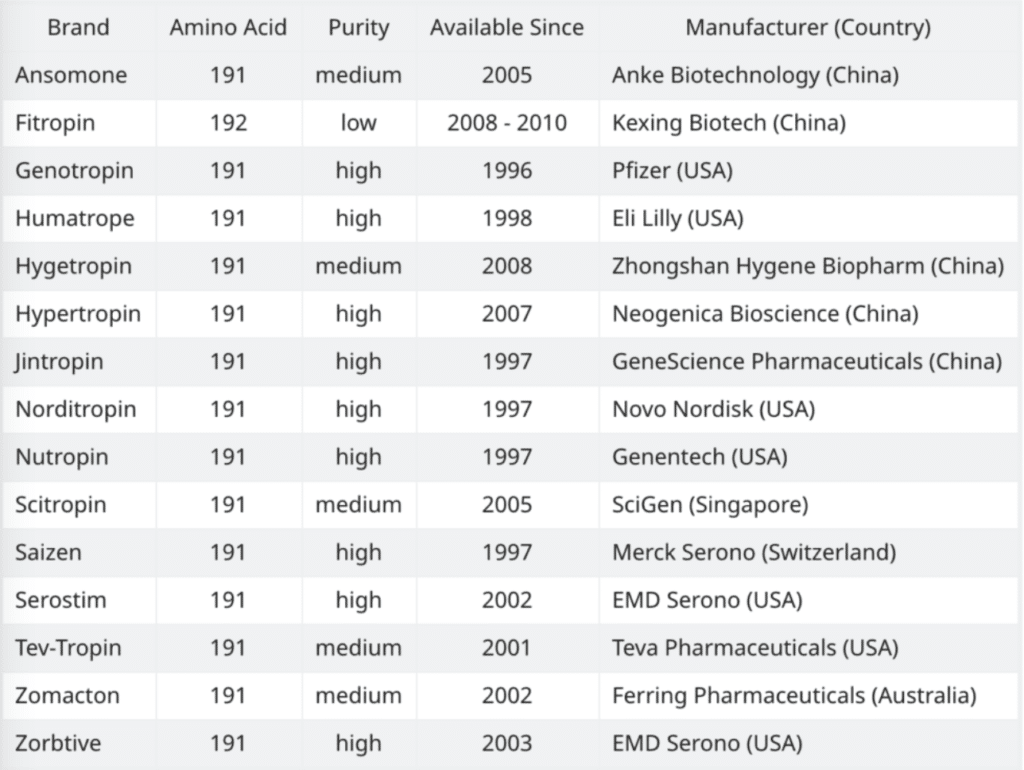
Unfortunately, as I said earlier, the only “legit” hGH you will find comes in the form of FDA or other International Big Pharmaceutical approved formulations:
(Source)
And for the most part ‘on paper’ they’re the exact same — very minute differences in formulation, some being approved for more disease states than others:
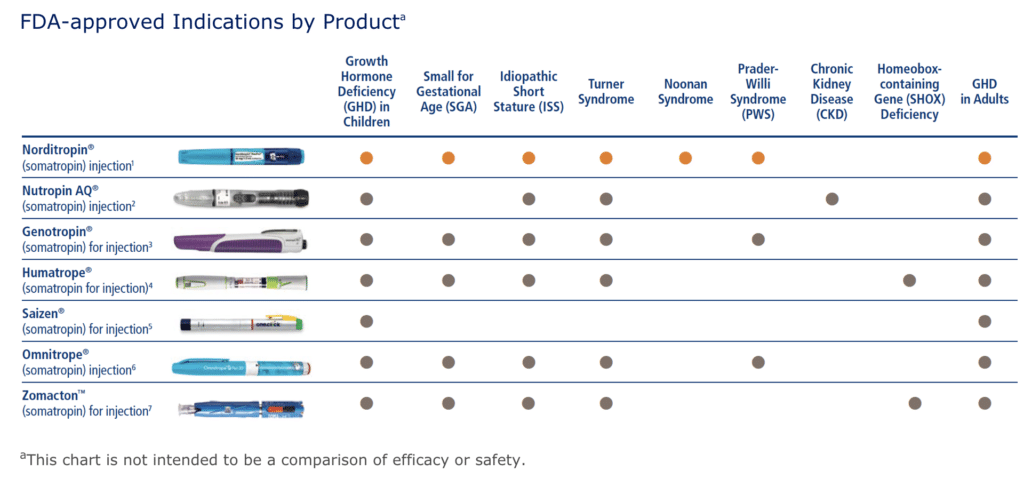
(Source)
But in actual real world usage reported from individuals in the life extension community, Genotropin and Norditropin stand out as the highest quality hGH formulations available.
Unless you can obtain one of these legit pharmaceutical grade brands, you’re likely forced to use a generic and Chinese form (sometimes 192 amino acid sequenced which is likely to lead to anti-body build up over time) hGH.
Or even worse, completely fake hGH altogether.
Even worse news for anyone reading this article, many of these pharmaceutical hGH brand names are routinely counterfeited. (In fact counterfeiting pharma hGH is a huge business.)
So to wrap up this deep and informative article, what do I personally recommend?
Ultimate Option: If you are an aging Man or Woman (over the age of 40) and you live where Genotropin or Norditropin are legally available (and you can afford a prescription), my recommendation is to pick one utilizing the dosages previously (as either a Man or a Woman) listed in combination with Hormonal Optimization, Dessicated Thyroid, Metformin and a diet emphasizing insulin controlled living.
OCTOBER 2021 UPDATE: I was recently introduced to this company in Thailand that offers Pharmaceutical HGH (i.e. Genotropin and Norditropin pens) at a super-discounted price.
For those of you where it is legally acceptable to purchase, click here!
NOTE: Please check the laws of your country before placing an order. It is illegal to use or purchase GH in the USA without a Doctor’s prescription.
Option For Most People: Due to pharma grade Tesamorelin only being available by prescription (Egrifta), I’d recommend using Ipamorelin and or in combination with CJC-1295 without DAC. (If any man can legally obtain pharma grade Tesamorelin, I’d use this in isolation over Ipamorelin due to its ability to preferentially burn fat off the midsection.
For Women, stick with Ipamorelin due to its low side effect profile and long understood and studied benefits as listed above.
Jay’s Comment about cycling these agents: I don’t think any Peptide cycle should be longer than 8-12 weeks in order to avoid or minimize antibody formation.
If one is using hGH, 6 months on (maximum) with 2-3 months off in between the next go round.
Both Ipamorelin and CJC-1295 are available at BioLongevity Labs.
(Use code JAYC to get 15% off your order)
You now know everything there is to know about choosing to use Human Growth Hormone (hGH) versus Therapeutic Peptides and the importance of keeping your human growth hormone production fully optimized for decades to come.
PS – When you’re ready to accelerate your journey towards supreme health, make sure you join My Fully Optimized Health Private Membership Group.
It’s your greatest opportunity to fully optimize your health, gain total access to myself and Daniel kelly, and network with high-level men looking to 10X their life.
You’ll also get access to our best-selling books and webinars for free, state-of-the-art testosterone optimization, cutting-edge research on peptides and supplements, and our “black book” rolodex of the world’s best hormonal health physicians.
And as always…


