Written by Jay Campbell
Written by Jay Campbell


Long-time followers of the Jay Campbell ecosystem KNOW I don’t frequently attend “biohacking” conferences.
Rarely do I go as an attendee, and it’s even rarer for me to be selected as a guest lecturer.
(The last time I did the latter was at SWIS 2018 in Toronto, Canada to talk about testosterone resistance syndrome)
I usually turn a blind eye to these kinds of gatherings as they’re nothing more than quack allopathic doctors who are several years behind the curve.
Talking about how to “manage” preventable disease states, debating principles of exercise and nutrition solved decades ago, and making hour-long presentations out of useless topics you could summarize on a single index card.
However… I AM convinced there might be an annual health optimization conference finally worth attending in the near future.
That would be none other than the Scientific Sessions run and hosted by the American Diabetes Association (ADA).
Especially for anybody and everybody who is even remotely interested in the GLP-1 peptide landscape.
This year’s conference was an explosion of must-read intel if you want to maximize your use of agents like Tirzepatide and Retatrutide.
Keep reading and you’ll see my hand-picked selection of the best info to come out of ADA’s Scientific Sessions this year!
What Are The ADA Scientific Sessions?
Taken straight from the press release on the official ADA website announcing the conference details:
“The ADA’s 84th Scientific Sessions, the world’s largest scientific meeting focused on diabetes research, prevention, and care, will be held in Orlando, FL [at the Orange county Convention Center] on June 21-24 [2024].
More than 11,000 leading physicians, scientists, and health care professionals from around the world are expected to convene both in person and virtually to unveil cutting-edge research, treatment recommendations, and advances toward a cure for diabetes.
Attendees will receive exclusive access to thousands of original research presentations and take part in provocative and engaging exchanges with leading diabetes experts.”
Over 2000 original research presentations were delivered, along with over 200 live sessions where chosen speakers could deliver their findings both in-person and live via Internet broadcast.
Given the popularity of this conference, the next 3 years already have their locations and times fully booked out:
- 85th Scientific Sessions: June 20-23, 205 at the McCormick Place Convention Center in Chicago, IL
- 86th Scientific Sessions: June 5-8, 2026 at the Ernest N. Morial Convention Center in New Orleans, LA
- 87th Scientific Sessions: June 18-21, 2027 at the Walter E. Washington Convention Center in Washington, DC
Here are some helpful links if you want to see a quick recap of what went down at the 84th Scientific Sessions
- Video highlights from the Australian Diabetes Society (ADS) for all four days of the conference from keynote speakers
- The schedule-at-a-glance for the conference, along with a full breakdown of each day’s presentations and activities
- Healio’s on-the-floor interviews with select attendees and what they discovered
- The European Association for the Study of Diabetes (EASD) compiled their favorite conference highlights from Day 1, Day 2, Day 3, and Day 4
Last but certainly not least, the ADA was kind enough to share a VERY comprehensive list of every single poster presentation, oral seminar, and publication presented at the 84th Scientific Sessions.
I strongly encourage you to browse the vast sea of new findings released by the researchers working hard to push the envelope of what’s possible for treating obesity and diabetes.
Why Biohackers Should Care About The ADA’s Scientific Sessions
You may remember an article I released last year where I interviewed former healthcare executive Jason Horowitz about the possible future of weight loss drugs.
Right before the interview started, the groundbreaking news about Retatrutide’s profound weight loss effects was released.
Guess where from?
None other than the ADA’s 83rd Scientific Sessions, which took place on June 23-26, 2023 at the San Diego Convention Center.
Presented by Eli Lilly scientists (the company manufacturing Retatrutide), here’s a short recap of the findings:
- Patients lost an average of 24% of their body weight over 48 weeks with just once-a-week injections of 12mg Retatrutide.
- 25% of the subjects receiving 12mg weekly of Retatrutide lost over 30% of their body weight.

(Source)
And that was just ONE big reveal among many others in relation to the GLP-1 receptor agonists.
So you can bet everyone – from Big Pharma to your average biohacker ‘bro’ – is now paying VERY close attention to this conference and others like it.
Why?
The next 5-10 years of every major diabetes and/or obesity conference are going to be nothing but the largest platforms for…
- Promoting the hottest weight loss drugs in the pipeline, and
- Finding new diseases and conditions to be treated by existing weight loss drugs
Yes, there are going to be other things to talk about such as the rise of artificial intelligence (AI) and novel biotechnologies designed to provide diabetics with superior care.
But effectively, you’re better off viewing them as “GLP-1 conferences” (or “playgrounds for pharmaceutical companies” for those of us with a strong disdain for the modern sick-care system)
A Word Of Caution About Attending The Scientific Sessions
A dirty secret about professional health conferences is that they are SERIOUS money-makers.
When you rack up all of the costs for a single person to attend, it easily adds up to a few thousand dollars depending on the nature of the conference:
- Registration fees (sometimes existing members get a discount, and early bird prices are often available)
- Travel to and from the conference
- Hotel accommodations
- Expenses during the conference (meals, travel within the city, etc.)
- Upgrades to “VIP” packages that provide more content and exclusive private access to select individuals
And for any budding physician, these conferences are convenient ways to take time off work and fulfill their Continuing Medical Education (CME) credits:
“CME refers to educational events that have been approved for CME credits. CME credits are important to physicians because some states require a specified number of credits annually to maintain medical licenses, and because most hospitals require a specified number of credits for their physicians to remain credentialed to see patients”
Not to mention these conferences tend to be extremely restrictive in terms of deciding what content the general public has access to.
In the case of the ADA’s 84th Scientific Sessions, virtual livestream access alone will cost you a pretty penny:
So if you’re a non-medical professional who simply has a strong passion for GLP-1 peptides, here’s what you can expect to pony up:
- $665 for access to the livestreams and nothing else
- Which you can only get WITH an additional $336 fee to become a member of the ADA
A cool $1,001.00 that doesn’t come with any bonuses or add-ons.
And now you can see how these conferences quickly become lucrative sources of income for the allopathic medical system.
There’s FAR more money to be made from extracting thousands of hard-earned dollars from physicians in exchange for “networking” and “education”.
(As if they don’t already put up with enough crap from all the administrative fees and procedures they suffer through just to keep their licenses)
Consider it the modern-day gold rush where you make 100x more from selling the shovels used to dig up the gold than actually digging up gold itself.
With tens of thousands of these conferences happening every year, one has to wonder if “the conference industry is vulnerable to the accusation that it is directed more towards profit for the organiser and invited speakers than necessarily and primarily towards benefit to the attendees and their clinical and academic work” (Source).
When you also factor in the direct or indirect support from Big Pharma companies with a vested interest in promoting their own medications/devices, one has to wonder if these conferences are truly created and run with the greater good in mind.
Nevertheless, enough info gets released thanks to the invention of social media.
Through hashtags on X/Twitter such as #ADA2024, #ada2024 and #ADASciSessions, scientists and clinicians were able to share all the info shared on the ground floor in real-time.
But that’s enough rambling from me… let’s dig into the MUST-KNOW intel uncovered at this year’s Scientific Sessions!
What We Learned About GLP-1 Receptor Agonist Peptides
Risk Of Suicide And Self-Harm
(Source)
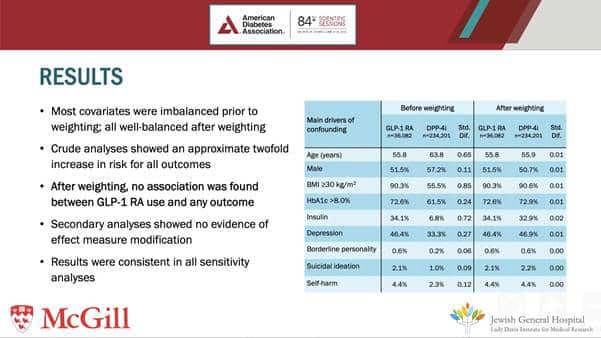
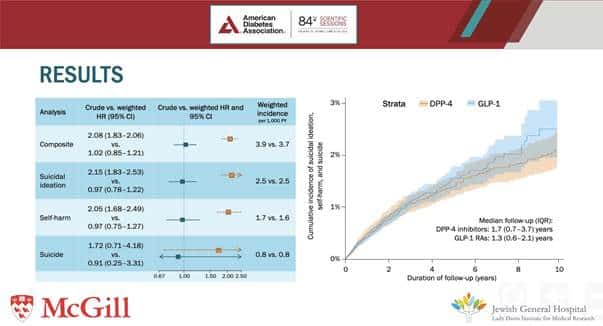
In this poster presentation, researchers went through data from the Clinical Practice Research Datalink (CPRD) located in the United Kingdom.
They looked at a cohort of type 2 diabetics who used either GLP-1 peptides (234,186) or DPP-4 inhibitors (36,083) between January 2007 and December 2020.
What they found:
- “The use of GLP-1 RAs was not associated with an increased risk of suicide or self-harm in this large, population-based study from the United Kingdom”
- “Increased reporting of thoughts of suicide and self-harm are likely due to confounding factors rather than a causal relationship”
Because there’s only the abstract available in combination with these two pictures, it is even more difficult to ascertain exactly what is going on here.
How many report of self-harm and suicide are directly attributable to Semaglutide (Ozempic/Wegovy), Tirzepatide (Mounjaro/Zepbound), or Retatrutide?
Is this something more common amongst the earlier GLP-1 peptides (Exenatide, Liraglutide, etc.)?
We’ll have to wait and see.
I should also note that generally, there are higher rates of depression and other mental health conditions among diabetics compared to the general population
A New Investigative Target For GLP-1 Peptides?
I thought this slide taken from an unlabeled presentation was interesting:
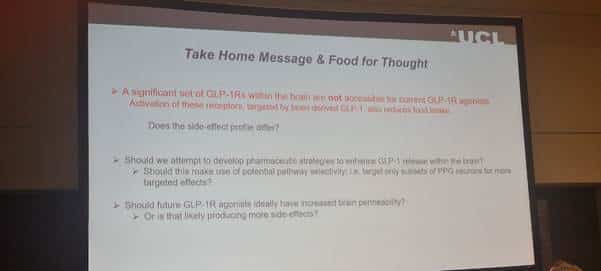
(Source)
“A significant set of GLP-1 receptors within the brain are NOT accessible for current GLP-1 receptor agonists… activation of these receptors also reduces food intake”
The last point about future GLP-1 peptides having increased brain permeability is relevant, given Semaglutide cannot directly cross the blood-brain barrier (BBB).
While there is the likelihood of side effects, it may be entirely possible to see different health benefits expressed differently.
For instance, there could be a better or worsened suppression of appetite. Or perhaps a stronger reduction in addictive behaviors.
Something for researchers to consider when manufacturing the next wave of weight loss drugs.
A New Ray Of Hope For Diabetic Americans
This headline also caught my attention when I was searching for breaking news from the 84th Scientific Sessions:
“An analysis of over 2.5 million patients with type 2 diabetes shows newer GLP-1 RAs [including dulaglutide, once-weekly or oral semaglutide, and tirzepatide] are linked to lower hemoglobin�?A1C (HbA1c) levels… and greater proportion of patients achieving an HbA1c less than 7%”
And the picture attached to the study told the whole story.
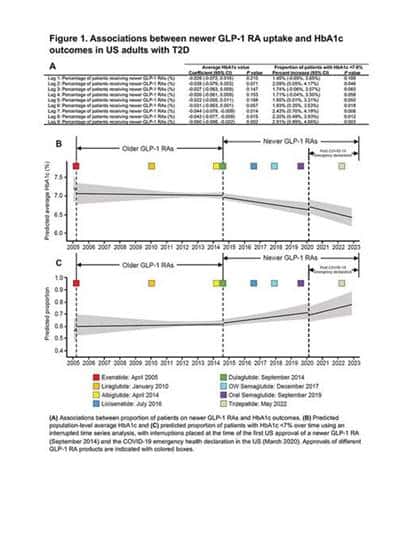
(Source)
The study looked at 2,508,308 patients with type 2 diabetes who had used Dulaglutide, Oral Semaglutide, Subcutaneous Semaglutide, or Tirzepatide.
And the data was leveraged between January 2004 and December 2022 from the Optum Clinformatics Data Mart.
To put the results in text, in case the graph doesn’t make it evident:
“…an increasing number of patients receiving new GLP-1 receptors agonists was associated with significant decreases in population-level HbA1c at 7 to 9 months (P�?<.05) and significant improvement in the proportion of patients with an HbA1c of less than 7% at 2 months and at 5 to 9 months (P�?<.05).
In the interrupted time series analysis, results suggest the introduction of newer GLP-1 receptor agonists was associated with decreased mean HbA1c and an increase in the proportion of patients with HbA1c of less than 7%.”
GLP-1s For Parkinson’s Disease?
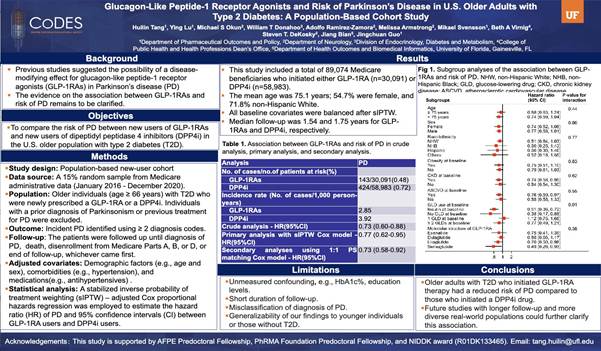
(Source)
In case the text from the poster above is too small to read:
“Older adults [>66 y/o] with type 2 diabetes who initiated GLP-1RA therapy had a reduced risk of Parkinson’s Disease compared to those who initiated a DPP4i drug [-33%]”
Some notable takeaways from this study:
- Administrative data was pooled from 89,074 Medicare beneficiaries who initiated either a GLP-1(n=30,091) or DPP4i (n=58,983) between January 2016 and December 2020
- “A significantly lower risk of PD was observed among those using insulin at baseline and those with no GLD (glucose-lowering drug) use at baseline, while no significant difference was detected among the groups using 1 GLD at baseline and ≥ 2 GLDs at baseline.”
Seems as if using MORE drugs may not necessarily be better in the context of treating Parkinson’s Disease with a GLP-1.
It might be more optimal to take one superior GLP-1 as opposed to using a combination of less powerful drugs.
GLP-1s Are In Desperate Need Of PROPER Body Composition Analysis
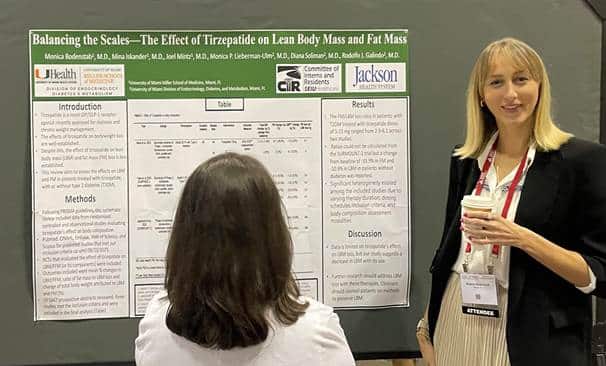
(Source)
I was unable to get a high-quality and unblocked version of this poster, but luckily the abstract and the accompanying table are available online.

“This [systematic] review aims to assess the effects on LBM and FM in patients treated with tirzepatide, with or without type 2 diabetes (T2DM).”
“…[we] included data from randomized controlled and observational studies evaluating tirzepatide’s effect on body composition. The ratio of FM/LBM loss was then assessed.”
“Of 5847 prospective abstracts, three studies were included in the final analysis (Table 1). The FM/LBM loss ratio in patients with T2DM treated with tirzepatide doses of 5-15 mg ranged from 2.9-6.1 across two studies. Ratios could not be calculated from the SURMOUNT-1 trial but a change from baseline of -33.9% in FM [fat mass] and -10.9% in LBM [lean body mass] in patients without diabetes was reported.”
“Data is limited on tirzepatide’s effect on LBM loss, but our study suggests a decrease in LBM with its use. Further research should address LBM loss with these therapies”
A couple of things to note…
First, the table clearly shows that every study analyzed has an end result of approximately 3 kg of fat mass lost per 1 kg of lean body mass lost (on average).
Is this ideal? Absolutely not, and I would personally like to see a better ratio.
But just from this crude analysis alone, there is clearly a strong trend in the direction of losing more fat than muscle during pharmacological-induced weight loss from Tirzepatide.
As registered dietitian Maureen Chomko said during one of the symposiums:
“Ms. Chomko also emphasized the importance of setting realistic expectations for the patient and educating them on the need for long-term treatment with incretin therapies.
Good nutrition, physical activity, adequate sleep, managing effects of other concurrent medications, and mental health can help patients stay on these medications and optimize their clinical benefits, she said.
For instance, as patients on incretin therapies often tolerate a lower variety of foods, they need may need to add B12, iron, calcium, and/or other supplements.
Patients on incretin therapies also may benefit from muscle mass-preserving physical activity, as muscle loss concomitant with overall weight loss may be a concern.“
Another published abstract presented at the 84th Scientific Sessions highlights the importance of the bolded point in a retrospective analysis of 53 people with type 2 diabetes.
These patients, whether on a GLP-1 (n=32) or not (n=21), followed a 12-week multidisciplinary structured intensive lifestyle intervention (sILI):
- 360 minutes of exercise per week, with greater emphasis on strength exercises
- Following�?“a hypocaloric structured medical nutrition therapy plan with increased protein intake to 1-1.5 gm/kg of adjusted body weight”
- “Body composition was analyzed by bioelectrical impedance”
The patients on a GLP-1 lost 7.4±4.5 kg in bodyweight and lowered their A1C�? by 0.84%±1.1%, with no changes in fat-free mass.
The patients NOT on a GLP-1 lost 6.2±5.4 kg in bodyweight and lowered their A1C�? by 1%±1.06%, with 1.4±2.6 kg of fat-free mass lost.
But across all three variables (body weight lost, A1C levels, fat free mass lost), the researchers state there was no difference between both groups over time.
In conclusion, the researchers stated:
“….increasing protein intake and strength exercises, as part of sILI, may mitigate the deleterious effect of GLP-1RA on muscle mass in patients with T2D.
These results support recommending an increase in protein intake and incorporation of strength exercises when GLP-1RA is prescribed for patients with T2D to minimize muscle mass loss.
Further research is needed to validate these findings in a randomized prospective study.”
Obviously, there are many improvements I would like to see with these types of studies.
A superior method of body composition analysis should be used — a BOD POD (hydrostatic weighing would be best), although a DEXA scan may be the more clinically practical option despite its higher error margin.
And the protein intake was absurdly low: A bare MINIMUM of 1 gram per pound of lean body mass should be used, and even higher protein intakes of 1.25 grams per pound of lean body mass would be optimal to preserve muscle tissue.
But at least the GLP-1 prescribing docs are waking up to what has been brain-dead common sense to bodybuilders for over 50 years.
The Short And Sweet Summary Of Managing GLP-1 Side Effects
(Source, Day 3)
Endocrinologist Dr. Beverly G. Tchang presented a talk at the “Severe GLP-1 RA Side Effects in Obesity Treatment – Fact or Fiction?” symposium.
Specifically, she “reviewed practical guidelines for clinicians and patients on managing GLP-1-related side effects.” (Source)
Although the full talk is only available to people who paid for virtual live stream access, the following three images summarize the key takeaways from Dr. Tchang’s presentation:
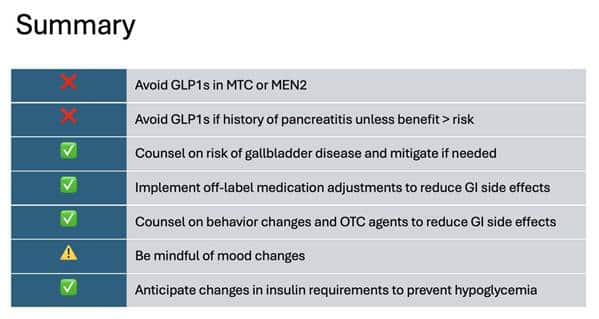
(Source, MTC = medullary thyroid cancer, MEN2 = multiple endocrine neoplasia type 2)


(Source)
I wonder if someone has spent the last two years screaming from the rooftops about everything seen above.
Or perhaps made a comprehensive video course telling you exactly what NOT to do on GLP-1 peptides. 😉
What We Learned About Semaglutide
Improving Symptoms Of Heart Failure Induced By Obesity
Results from the STEP-HFpEF (Semaglutide Treatment Effect in People with Obesity and HFpEF) program (along with a secondary analysis) were presented at the 84th Scientific Sessions.
(HF = heart failure, HFpEF = heart failure with preserved ejection fraction)


The key takeaways are as follows:
- The study involved 1,145 participants with obesity-related HFpEF over 52 weeks (570 women, 575 men)
- Two groups were involved: A placebo group, and a group receiving 2.4 mg of Semaglutide once a week
- Semaglutide “improved HF-related symptoms, physical limitations, exercise function, and reduced inflammation and natriuretic peptides regardless of sex” along with lowered systolic blood pressure and waist circumference compared to placebo (Source)
- A statistically significant reduction in body weight was observed overall, along with a statistically significant difference in weight loss between the sexes (-9.6% for women, -7.2% for men) (Source)

(Source)
Here’s the real takeaway:
Given the larger weight loss in women did not necessarily result in MORE health benefits compared to men, there is a strong suggestion that the improvements in obesity-related heart failure induced by Semaglutide may be independent of weight loss itself!
This study also leads to asking the following questions:

(Source)
Improvements In Kidney Disease Parameters
The results from the FLOW (Evaluate Renal Function with Semaglutide Once Weekly) clinical trial were published and presented at the 84th Scientific Sessions.
Funded by Novo Nordisk, the official clinical trial details can be found here.
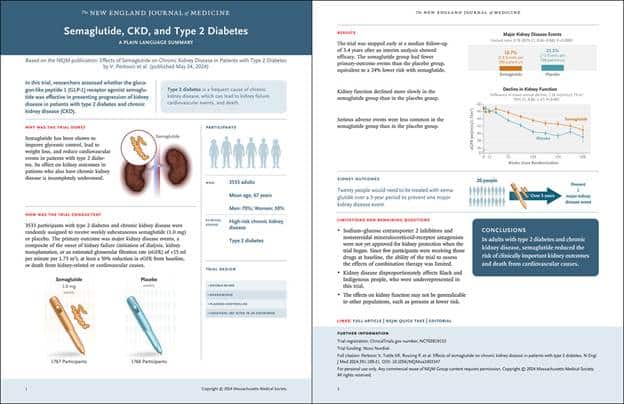
To sum it up in one sentence:
Among patients with chronic kidney disease (CKD) and type 2 diabetes (T2D), once-weekly subcutaneous semaglutide [1 mg, n=1,767] was superior to placebo [n=1,766] in improving renal and CV [cardiovascular] outcomes over a median follow-up of 3.4 years… the benefits of semaglutide in improving renal outcomes were consistent in patients with/without baseline SGLT2i [sodium-glucose cotransporter 2 inhibitor] use” (Source)
Here are some other notable conclusions from the trial:
- Significant adverse effects were fewer in the semaglutide group (49.6%) vs. placebo (53.8%)
- A 20% reduction in relative mortality was observed in the semaglutide group relative to the placebo group
- “The risk of the primary outcome [composite of kidney failure, ≥50% estimated glomerular filtration rate reduction, kidney death or CV death] was 24% lower in all participants treated with semaglutide versus placebo” (Source)
- “Semaglutide benefits were observed for adults with type 2 diabetes and chronic kidney disease whether or not they used SGLT2 inhibitors… [but] the FLOW trial was not powered to observe effects for those on SGLT2s” (Source)
Improvements In Cardiovascular Outcomes
Additionally, the results of the Semaglutide Effects on Cardiovascular Outcomes in People With Overweight or Obesity (SELECT) trial were presented:
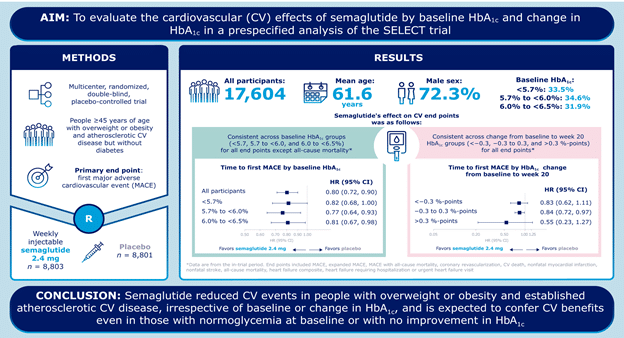
Some important things to note about the trial:
- “…long-term semaglutide increases regression to biochemical normoglycemia and reduces progression to biochemical diabetes (73% reduction in relative risk over four years) but does not slow glycemic progression over time“, with a mean body weight loss of 8.9% over 65 weeks (Source)
- The cardioprotective effects observed with semaglutide use are not dependent on HbA1C levels.�?
- “About two-thirds of the 17,604 participants in the global trial had prediabetes at baseline and one-third had normoglycemia. All had established cardiovascular (CV) disease, and the mean body mass index (BMI) was 33… Regardless of body weight or BMI at baseline, semaglutide reduced progression to diabetes” (Source)
- “The SELECT trial established semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist, as effective in reducing cardiovascular events by 20% in people considered to be overweight or obese who have cardiovascular disease without diabetes” (Source)
Even though I no longer recommend the use of Semaglutide, it is still a very useful investigational drug as it gives us clues about what we can expect with updated GLP-1 peptides such as Tirzepatide and Retatrutide.
What We Learned About Tirzepatide
Safe & Effective For The Treatment Of Type 1 Diabetes

(Source)
From the presentation abstract:
“This is a retrospective study of 52 adults with T1D treated with tirzepatide for obesity. Exclusion criteria: tirzepatide use for <3 months, use of other antiobesity medications, and active malignancy.”
“In adults with T1D, tirzepatide led to significant weight loss, better diabetes control, and lower insulin requirements without causing severe hypoglycemia or DKA [diabetes ketoacidosis] over the course of up to 12 months. The side effect profile mimicked what has been reported. These data support the effectiveness and safety of tirzepatide for the treatment of obesity in adults with T1D”
Similar results were found in a separate retrospective study presented at the conference:
“This was a retrospective single center real-world study in 62 adult OW [overweight] /OB [obese] patients with T1D who were prescribed tirzepatide and followed for one year. The control group included 37 T1D patients (computer matched) with OW or OB who were not using any weight loss medications during the same period.”
“The mean baseline age, duration of diabetes and HbA1c were similar in the 2 groups, while BMI and weight were higher in cases. There were significantly larger declines in BMI and weight in cases than controls across all time points. HbA1c decreased in cases as early as 3 months which was sustained throughout 1-year follow-up. There was no reported increase in severe hypoglycemia or diabetic ketoacidosis throughout the study duration.
“In this pilot off-label use study, we conclude that tirzepatide facilitated an average 18.5% weight loss and improved glucose control in OW/OB patients with T1D”
And when compared head-on against Semaglutide for type 1 diabetes, it appears as if Tirzepatide provides slightly better reductions in blood glucose levels while leading to significantly more weight loss.
Treating Obstructive Sleep Apnea In Obese Patients
These were two pivotal Phase 3 clinical trials (SURMOUNT-OSA) whose results were published during the conference:
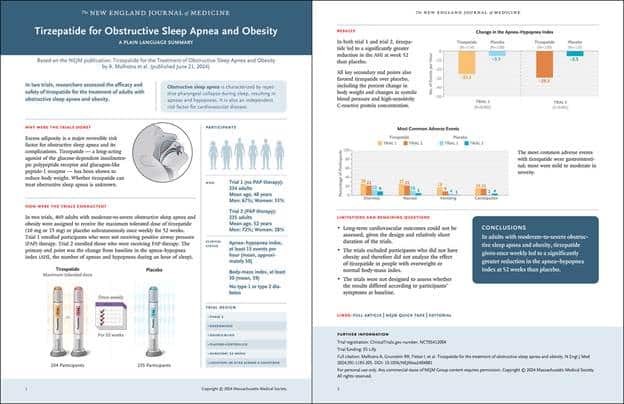
There’s a lot to break down here, so I’ll summarize all the info as succinctly as possible (taken from here and here):
- Study 1:
- “involved patients who could not or did not want to use positive airway pressure (PAP) therapy,”
- “A total of 234 individuals were included in study 1, with 114 receiving tirzepatide and 120 receiving placebo… and a mean AHI [apnea-hypopnea index] of 51.5 events per hour”
- “use of tirzepatide was associated with a change in AHI�?of- 27.4 events per hour (95% CI, −31.6 to −23.2) from baseline to week 52 compared to −4.8 events per hour (95% CI, −9.3 to −0.3) with placebo”
- “disease resolution was achieved by 43.0% of patients receiving the highest dose of tirzepatide in study 1”
- “events occurring at a greater frequency than placebo included diarrhea (26.3% vs 12.5%), nausea (25.4% vs 10.0%), and vomiting (17.5% vs 4.2%)”
- Study 2:
- “included patients who were on and planned to continue PAP therapy”
- “A total of 235 individuals were included in study 2, with 120 receiving tirzepatide and 115 receiving placebo… and a mean AHI of 49.5 events per hour.”
- “…use of tirzepatide was associated with a change in AHI of −30.4 events per hour (95% CI, −34.3 to −26.5) from baseline to week 52 compared to −6.0 events per hour (95% CI, −10.3 to −1.6) with placebo”
- “disease resolution was achieved by 51.5% of patients receiving the highest dose of tirzepatide in study 2”
- “events occurring at a greater frequency than placebo included diarrhea (21.8% vs 8.8%), nausea (21.8% vs 5.3%), and constipation (15.1% vs 4.4%).”
Other worthwhile improvements observed included the following:
“Notable changes of CV risk factors included reductions in body weight (18 percent in Study 1 and 20 percent in Study 2) and improvements in systolic blood pressure (-9.6 in Study 1 and -7.6 in Study 2).
The number of participants who stopped being indicated for CPAP treatment was also improved with tirzepatide compared to placebo, and the Patient-Reported Outcomes Measurement Information System (PROMIS) scores for sleep-related impairment and sleep disturbance were improved”

(taken from the study itself)
Observed Effectiveness In The Real World
One presentation abstract looked at 2,247 patients with Type 2 Diabetes who started Tirzepatide between May 2022 and August 2023.
After a 6-month follow up from the initiation of Tirzepatide, here is what researchers found:
- Overall changes in HbA1c was -1% and overall mean weight loss was -6.3 kg
- For people with a baseline HbA1C above 7% : HbA1C went down by -1.4% and weight went down by -5.8 kg
- For people who did not have prior use of GLP-1 medications: HbA1C went down by -1.3% and weight went down by -8.1 kg
A poster summary of this retrospective cohort study can be found below:
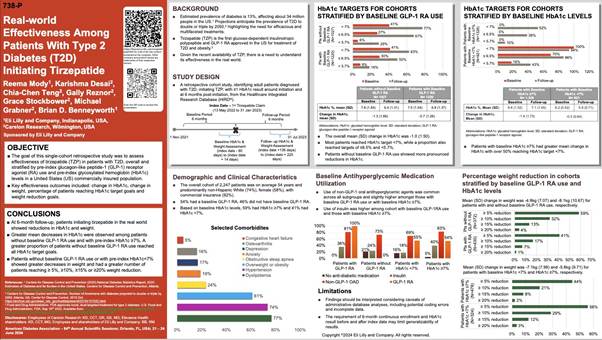
(Source)
Another retrospective study looked at the real-world effectiveness of Tirzepatide in overweight/obese patients WITHOUT type 2 diabetes.

(Source)
“Among the 699 AOM [anti obesity medication] eligible adults without TD2 diagnostic codes who filled a prescription for tirzepatide, most were female (77.1%), White (81.1%), mean age 47.2 years, mean BMI 38.3 kg/m2, mean weight 109.3 kg (241.0 lbs), and of those with a 6th�?prescription fill (n=405), 44.4% was for ≥10 mg.
At least one ORC [obesity-related comorbidity] was reported in 86.4% of patients. Hypertension (44.5%), dyslipidemia (43.6%), and anxiety (35.8%) were the most common ORCs.
Of the 68.8% (n=481) who were persistent for ≥6 months, weight data were available at baseline and 6-months post-index for n=199; 88.4% had ≥5%, 68.8% had ≥10%, and 36.7% had ≥15% weight reduction at 6-months post-index. The average weight reduction was 12.7% (14.1 kg [31.1 lbs]).”
While these results are far from definitive, it is reassuring to see early real-world data more-or-less match what has been observed in tightly controlled clinical trial settings.
What We Learned About Retatrutide
Improved Markers Of Insulin Sensitivity
From the presentation abstract:
“… [we] evaluated fasting biomarkers from two Ph2 double-blind randomized placebo-controlled trials: in T2D [type 2 diabetes[ (281 subjects, 36-wks) and in OB [obesity without T2D] (338 subjects, 48-wks).
Homeostatic model assessment (HOMA2)-IR index (insulin), a measure of insulin resistance, decreased over time from baseline with RETA�? [retatrutide] 12 mg reaching reductions of 39% in T2D at 36 wks and 52% in OB at 48 wks.
Adiponectin, a marker of insulin sensitivity, increased with RETA from baseline up to 52% in T2D and up to 70% in OB, (p<0.001).”
“Proinsulin and proinsulin/C-peptide ratios, measures of beta-cell stress and dysfunction, decreased from baseline with RETA, by up to 71% and 62%, respectively, in T2D (p<0.001).”

Improvements In Lipid Profiling
From the presentation abstract:
“Adult participants with obesity (BMI ≥30 kg/m2), or overweight (BMI ≥ 27 kg/m2) with a weight related comorbidity, were randomized to RETA [retatrutide] 1, 4, 8, 12 mg or PBO [placebo] for 48 weeks.
…An increase in 3-hydroxybutyrate (3-HB) was noted after 24 wk, accompanied by an increase in 3-hydroxybutyrylcarnitine (C4OH), acetylcarnitine-to-free carnitine ratio (C2/C0), and medium-chain ACs.
The decrease of TGs [triglycerides] at 48 wk was bias towards short-chain and saturated species.
RETA 12 mg decreased total dihydroceramides (DhCers) at 48 wk by −20.1%, p-value <0.001. The increase in ketone body and C2/C0 observed after 24 wk is suggestive of adipose tissue lipolysis and reliance on fat oxidation”
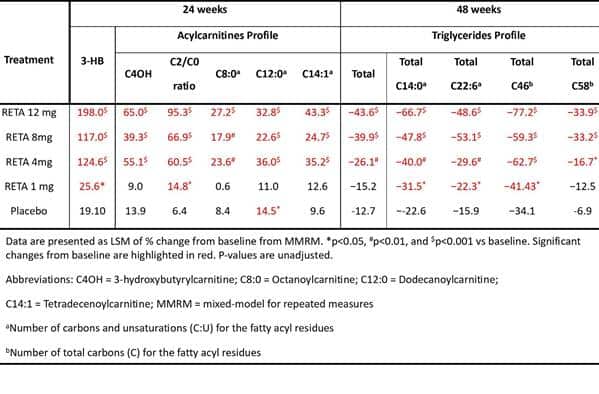
The increase in ketone bodies and the implication of lipolysis is something I didn’t expect, and it certainly has beneficial implications for patients following a ketogenic diet.
But it’s clear that several key biomarkers of health improve with the use of Retatrutide, showing us it’s far more than just a one-trick pony.
Improvements In Kidney Parameters for Obese and Diabetic Patients
From the presentation abstract:
“Data from all participants in 2 phase 2 studies were included: T2D (N=281): RETA [retatrutide] (0.5, 4, 8, 12 mg) vs dulaglutide 1.5 mg vs PBO [placebo] (N=45-50/arm); OB [obese] (non-T2D; N=338): RETA (1, 4, 8, 12 mg) vs PBO (N=62-70/arm).
Assessments included CKD-EPI creatinine eGFR (Cr-eGFR), cystatin C-based eGFR and urine albumin-to-creatinine ratio (UACR).
…At 36 wks in T2D, no difference was observed in Cr-eGFR between all RETA groups and PBO; UACR was significantly reduced vs PBO with RETA 12 mg.
In OB, RETA 8 and 12 mg increased Cr-eGFR and decreased UACR compared to PBO at 48 wks. Results were similar when GFR was estimated from cystatin C.
Blood pressure (BP) was significantly reduced in both studies.
RETA 8 and 12 mg increased eGFR in people with OB but not in those with T2D. UACR and BP were reduced vs PBO with higher doses of RETA in both trials”
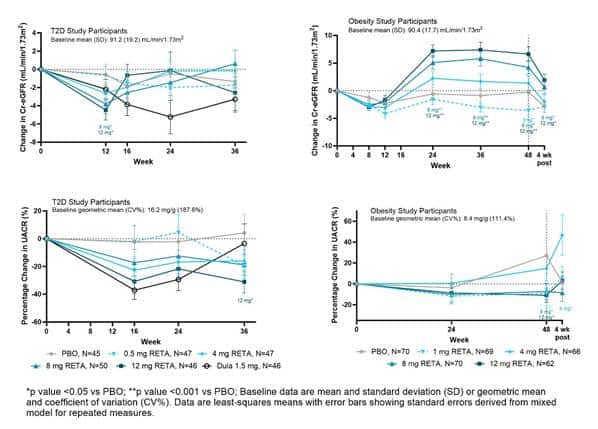
It’s worth noting that drops were observed in both systolic (SBP) and diastolic blood pressure (DBP):

(Source)
From the Twitter thread I took this picture from, one commenter had the following to say:
“[These results are] probably an effect of weight loss combined with indexing eGFR [estimated glomerular filtration rate] to standard BSA [body surface area] of 1.73M2. eGFR, regardless of biomarker, will increase with weight loss (and BSA decline) when values are indexed to a Standard BSA”
Much more data should be collected to ascertain exactly what is happening here.
Improved Eating Behaviors

(Source)
In case you can’t read the conclusion:
“Higher doses of retatrutide significantly improved eating behaviors, such as overeating and perceived hunger, compared to placebo or dulaglutide in a dose-dependent manner in adults with type 2 diabetes at 36 weeks… conscious restriction of food intake improved more in the retatrutide group than in the placebo group”
This last finding was especially relevant to the hundreds of thousands of testimonials from GLP-1 users that their appetites are significantly reduced.
From the original presentation abstract:
“Adults with T2D were randomized to subcutaneous placebo QW [once weekly], DU [dulaglutide] 1.5 mg QW, or RETA [retatrutide] 0.5, 4, 8, or 12 mg QW for 36 weeks in this double-blind, double-dummy Phase 2 study. Eating behavior was assessed at baseline and Week 36 using the 51-item Eating Inventory comprised of three domains: Cognitive Restraint of Eating, Disinhibition, and Perceived Hunger.”
“At Week 36, adults treated with RETA 8 mg and 12 mg had significantly reduced Eating Inventory Disinhibition and Perceived Hunger scores vs. placebo. Adults treated with RETA 12 mg also had significantly reduced Disinhibition and Perceived Hunger scores vs. DU and a significantly reduced Cognitive Restraint of Eating score vs. placebo at Week 36.”

NOTE: All information presented by Eli Lilly at the 84th Scientific Sessions (posters, slides, etc.) can be found here.�?
What We Learned About Living A Fully Optimized Lifestyle
The Link Between BPA And Insulin Resistance
This headline made me fall out of my chair because we have KNOWN about the harmful impacts of endocrine-disrupting chemicals (EDCs) for decades.
But the study abstract says it all:
“Forty non-habitually active, healthy adults (22 F, 18 M; 21.3 ± 2.5 yr; 22.1 ± 2.3 kg/m2; 85% Non-Hispanic White) completed a 2-day baseline energy balance diet low in bisphenols during which urine, blood, and peripheral insulin sensitivity (i.e., glucose infusion rate/steady-state plasma insulin) via 120 min euglycemic hyperinsulinemic clamp technique (40 mU/m2/min; 90 mg/dL) were assessed.
Participants were then randomly assigned, in a double-blinded fashion, to a 4-day energy balance diet plus oral BPA administration at 50 μg/kg body weight (BPA-50) or 4-day energy balance diet plus oral placebo (PL) administration”
And here’s where it gets scary:
“Compared to PL urine BPA was significantly higher (P<0.05) following BPA-50.
From baseline to 4-days, peripheral insulin sensitivity significantly (P=0.01) decreased in BPA-50 (0.11 ± 0.01, 0.10 ± 0.01 mg/kg/min/uU/ml) and remained stable in PL (0.09 ± 0.01, 0.10 ± 0.01 mg/kg/min/uU/ml).”
This MATTERS if you are someone who is diabetic or at great risk for becoming diabetic, as the Europeans have already found out:
“This is no trivial observational study of correlations that would be easy to dismiss. Rather, it is a well-controlled, randomized clinical study of exposure to BPA in low doses. The exposure was only 50 μg/kg body weight for four days.
These are amounts the U.S. Environmental Protection Agency calls “safe.” But even at this low dose, it caused insulin sensitivity to drop significantly.”
Sadly, BPA exposure is almost unavoidable due to its presence in everyday items:
“BPA and other bisphenols are found in canned foods and plastics. BPA is one of the most widely used synthetic chemicals and we consume foods that are packed in this chemical. Most of BPA exposure comes from canned foods, and 93% of the US populations has detectable urine levels of BPA. We can limit BPA by reducing canned foods (or purchased BPA free cans) and plastic use.”
Losing Weight Decreases Your Risk Of Cancer If You’re Obese
Something like this shouldn’t be a revelation or a surprise to anybody with an ounce of common sense.

(Source)
More stats for those of you who still won’t listen:
“Overall, 78% of people with diabetes have clinical obesity. Obesity is�?linked to higher risks of at least 13 types of cancer due to excess estrogen and elevated insulin, including breast, kidney, ovary, liver, and pancreatic cancer”
And here’s the abstract detailing what should have been obvious from the get-go.
In short, 105,489 patients’ data was retrospectively analyzed from the Cleveland Clinic’s electronic health records between January 2000 and December 2022.
The researchers were tracking 13 obesity-related cancers while searching for 17 other types of cancer that were likely to occur as well.
Also, they tracked the association between the percentage change in BMI at 3, 5 and 10 years prior to the diagnosis of a given cancer.
From the abstract itself:
“Our results show reduced risk of developing obesity-related cancers with weight loss at 3 years (OR 0.99, 95%CI [0.984, 0.996]) and 5 years (OR 0.989,95% CI [0.983-0.995]), and for other types of cancer for all time intervals (ORs<1, P <0.001) (Figure 1a).
The risk was reduced for renal cell carcinoma (3 years), multiple myeloma (10 years), and endometrial cancer (3 & 5 years) among primary cancer endpoints (P<0.05) (Figure 1b)”
To really drive the point home:
“Adults also had lower odds for being diagnosed with any malignant cancer with each 1 percentage point decrease in BMI over a 3-year period (OR = 0.992; 95% CI, 0.989-0.996;�?P�?< .001), 5-year period (OR = 0.994; 95% CI, 0.991-0.997;�?P�?< .001) and 10-year period (OR = 0.991; 95% CI, 0.987-0.995;�?P < .001).”
Unfortunately, as per the course, researchers opined that “more data is needed”:
“Investigators indicated more research is necessary to evaluate if cancer risk is affected by the amount, rate, and weight loss method. Thus, future studies may focus on the effect of specific anti-obesity medications on reducing cancer risk.”
With where we are as a species, combined with the projected yet catastrophic death rate from obesity, it’s safe to say we’ve seen enough and waiting any longer will literally kill us all.
What We Learned About Potential Weight Loss Drugs In The Pipeline
To be frank, there were WAY too many new drugs presented for me to discuss all of them here.
I AM going to present what I thought were the three best announcements (and the agents you should be keeping a close eye on).
NA-931
From the presentation abstract covering this quadruple agonist (GLP-1, GIP, IGF-1, Glucagon):
“Insulin-like Growth Factor 1 (IGF-1) plays a major part in fuel metabolism and regulation of body composition… IGF-1 contributes to modulate glucagon secretion in which IGF-1 inhibits the ability of low glucose concentration to stimulate glucagon expression and secretion”
“Male diet-induced obese (DIO) mice were treated with daily subcutaneous injections of vehicle or one of novel triple IGF-1/GLP-1/GIP receptor agonists, NA-931, NA-932 and NA-933 (10 nmol/kg), for 14 days. Tirzepatide (10 nmol/ kg) as used as positive controls”
“NA-931 and its analogs produced significant reductions in BW in DIO mice. Effect sizes were comparable to those observed in the tirzepatide control group. The NA-931 Compounds have been shown to produce desirable changes to lipid profile, suggesting global cardiometabolic benefit, represent a promising therapeutic approach to metabolic disorders such as obesity, type 2 diabetes, and non-alcoholic steatohepatitis”
And from the official page of Biomed Industries, the biopharmaceutical company manufacturing NA-931:
- NA-931 can easily cross the blood-brain barrier, meaning it will be effective at small doses
- Available in an oral formulation (one capsule taken daily)
- No serious adverse events reported so far, implying it is well-tolerated and safe to use (and possibly has fewer side effects than existing GLP-1 targeting therapies)
- Currently in Phase 2B clinical trials
- Significantly lowers body fat while preserving muscle mass (NOTE: No official data has been presented to prove this claim yet)
Pemvidutide
From the presentation abstract covering the results of this GLP-1/glucagon dual agonist:
“MOMENTUM was a Phase 2, randomized, placebo-controlled trial of 391 subjects with overweight (BMI 27.0-29.9 kg/m2) and at least one obesity-related comorbidity or obesity (BMI >30.0 kg/m2) randomized 1:1:1:1 to pemvidutide (1.2, 1.8, 2.4 mg) or placebo administered subcutaneously weekly for 48 weeks [mean age, body weight, and BMI of 50 yrs, 105 kg, and 37 kg/m2]”�?
“…subjects receiving pemvidutide achieved mean weight losses of 10.3%, 11.2%, and 15.6% at the 1.2 mg, 1.8 mg, and 2.4 mg doses vs. placebo (2.2%), respectively (p<0.001 vs. placebo, all doses, Figure 1), with 51.8% and 32.1% of subjects at the 2.4 mg dose level achieving ≥15% and ≥20% weight loss and 48% of subjects having resolution of baseline obesity by trial conclusion”
” Subjects with elevated serum lipids at baseline had reductions of up to 55.8%, 20.0%, and 21.8% in triglycerides, total cholesterol and LDL at week 48″

There was also this press release from Altimmune, the pharmaceutical company manufacturing Pemvidutide, published at the same time the abstract above was presented:
“The full MRI-based body composition analysis included 50 subjects who received pemvidutide and showed that subjects in the pemvidutide groups had an average lean mass loss of 21.9% with 78.1% of weight loss attributable to fat.
In addition, pemvidutide resulted in robust reductions in serum lipids and improvements in blood pressure without imbalances in cardiac events, arrhythmias or clinically meaningful increases in heart rate.”
Very impressive when you consider these results in relation to Semaglutide and Tirzepatide:
- “Tirzepatide (SURPASS Trials): 25-30% of the weight lost was lean body mass, and 70-75% was fat mass”
- “Semaglutide (STEP Trials): 39% of the weight loss was lean body mass, and 61% was fat mass”
Again, keep in mind these studies DO NOT have patients following what would be considered a fully optimized lifestyle.
High protein intake, bone-bearing resistance training, healthier food selection, and living insulin-controlled, as Dr. Rudy Eberwein told us a long time ago.
HRS9531
From the presentation abstract presenting the Phase 2 clinical trial results of this novel GIP/GLP-1 agonist developed by Chinese pharmaceutical company Jiangsu Hengrui:
“249 Chinese adults with a BMI of 28-40 kg/m2 were randomized 1:1:1:1:1 to receive once-weekly subcutaneous injections of HRS9531 (1.0 mg, 3.0 mg, 4.5 mg, and 6.0 mg) or placebo for 24 weeks (24W)”
“participants in 1.0 mg, 3.0 mg, 4.5 mg, and 6.0 mg HRS9531 groups achieved weight reductions of 5.4%, 13.4%, 14.0%, and 16.8% respectively, as compared with 0.1% reduction in the placebo group. Moreover, the proportion of participants achieving ≥5% weight reduction was 52.0%, 88.2%, 92.0%, 91.8%, and 10.2%, respectively” (Source)
“HRS9531 outperformed placebo in lowering blood pressure, improving glycemic control, and reducing triglyceride levels. The least-squares mean changes from baseline to W24 in systolic blood pressure ranged from -4.46 to -8.33 mmHg in the HRS9531 groups (placebo: -0.41 mmHg) and in the waist circumference ranged from -5.14 to -12.73 cm in the HRS9531 groups (placebo: -1.82 cm).”
“No serious AEs were treatment-related and no participants discontinued treatment due to treatment-related AEs.”
And from another abstract presenting the Phase 1 clinical trial results involving the use of a single or multiple ascending dose (MAD):
“The most common adverse events were abdominal distension and nausea in SAD, and urine ketone body present and nausea in MAD; all considered mild to moderate in severity (mostly mild). No severe hypoglycemia or serious events occurred”
“In SAD [single ascending dose], body weight loss was dose-dependent and the maximal mean loss on D8 was 3.8 kg (4.9%) in 8.1 mg group. In MAD, the mean weight loss on D29 (after 4 wks treatment) ranged 4.3-7.7 kg (6.7%-9.3%) across 0.9-5.4 mg groups, and maximal loss (8.0 kg, 10.0%) occurred on D36 in 5.4 mg group”
“HRS9531 was well tolerated, had favorable PK [pharmacokinetics], and led to evident glucose decrease and body weight loss.”
The Future Of GLP-1 Targeting Drugs
Despite only covering a tiny fraction of what was presented at the ADA’s 84th Scientific Sessions, I AM confident in saying the future has never looked brighter for GLP-1 based weight loss medications.
The existing medications on the market continue to find novel uses for a growing number of chronic disease states.
The newer drugs in development promise to deliver even better results already seen in the real world: Faster weight loss, better biomarker improvement, more lean mass preservation, and fewer side effects.
But as I said earlier in this article: NONE of these drugs will lead to total health optimization without an insulin-controlled lifestyle.
A fact that very few doctors specializing in weight loss are aware of.
Only the select few equipped with the right knowledge of how these medications actually work, in combination with fundamental body recomposition principles, will experience long-lasting changes with GLP-1 peptides.
Without losing muscle, without any scary side effects, and without lifelong dependence on them.
Now, if you want to take your health optimization journey to the next level:
I invite you to join me and other like-minded biohackers in The Fully Optimized Health Private Membership Group.
This is where we dive deep into using peptides to optimize health, especially for those in their 30s and beyond.
We’re also talking about cutting-edge biohacking and the latest and greatest in elite health optimization strategies.
And don’t forget to check out our other premium educational content dedicated to helping you fully optimize your health:
Peptides Demystified – the step-by-step, A-to-Z system for newbies desiring to master peptide use for the first time and forever.
The Ultimate GLP-1 Video Masterclass – how to PROPERLY utilize the world’s most powerful weight loss drugs for enhanced fat loss and overall longevity.
The Modern Woman’s Peptide Course – a must-have resource for any woman seeking to become more feminine, sexier, leaner, and healthier through the use of peptides.
Life Enhanced�?– Unlock the secrets to TOTAL Mind-Body-Spirit Optimization as Hunter Williams and I teach you how to live at the tip of the spear.
30 Days 2 Shredz – Reprogram Your Mind and Body for Maximum Fat Loss in Minimum Time with our Optimized Fasting Protocol
See you on the inside!