 Written by Jay Campbell
Written by Jay Campbell



The GLP-1 peptide revolution has led us down a rather interesting path.
It seemed like yesterday when Semaglutide (a.k.a. Wegovy, Ozempic, Rybelsus) was the sole focus of dietitians, diabetes-focused physicians, and the biohacking community at large.
Nobody really knew or cared about the glucagon-like peptide-1 (GLP-1) hormone until people saw how harnessing its properties could lead to transformational health benefits.
But the anti-obesity drug landscape has radically changed in just a few short years.
We now have Tirzepatide, the co-agonist peptide targeting both GLP-1 and glucose-dependent insulinotropic polypeptide (GIP), which offers all the benefits of Semaglutide in a superior fashion.
Yet the fun doesn’t stop there.
Just when you think we’ve reached the pinnacle of what’s possible with weight loss medications, along comes Retatrutide.
If Tirzepatide is the “King Kong” of the GLP-1 peptide universe, Retatrutide wins out as “Godzilla”.
(Those who want to understand the monster-verse reference should go here to see the debate about the 2021 Godzilla Vs. Kong movie)
By targeting GLP-1, GIP, AND glucagon simultaneously, our previous paradigm of what is achievable through pharmacologically-induced weight has once again been shattered.
But BEFORE I can spill all the goods on (currently) the world’s best weight loss drug, I have to give you some background info.
This will be Part 1, where we go over the history of triple-agonist weight loss drugs that led to the idea and creation of Retatrutide.
In Part 2, we’ll review all the scientific data published to date about Retatrutide and show you how to use it safely and effectively for maximal fat loss.
Let’s start this long yet worthwhile journey!
Explaining The Retatrutide Hype
I AM sure many of you are well aware why the hype behind Retatrutide is both unsurprising and well-deserved
I mentioned it briefly in my article about the world’s best peptide stacks, when preclinical results released in 2021 showed its unquestionable superiority to both Tirzepatide and Cotatutide (a dual GLP-1/glucagon agonist).
Then you had Retatrutide’s Phase 2 clinical trial results released in the summer of 2023, where the highest dose (12mg injected subcutaneously once a week) led to a staggering 24.2% loss in body weight over 48 weeks.
Finally, the American Diabetes Association (ADA) 84th Scientific Sessions held last year revealed even more profound insights about what this triple-threat peptide can do in humans:
- Improve biomarkers of insulin sensitivity
- Better lipid profiling
- Improved kidney parameters in people with obesity and diabetes
- Greater conscious restriction of food intake, reduced overeating and less perceived hunger in adults with Type 2 Diabetes
Granted, these were all poster abstracts that are due to be published in peer-reviewed papers once the data is better analyzed and presented.
But whatever all the single and double receptor agonists were capable of doing up until now, Retatrutide smokes them out of the water across every measurable outcome.
Why Add On A Third Target Receptor, And Why Glucagon?
Yet as I was looking at all of the data on Retatrutide, something hit me…
What was the rationale behind the executive decision to add glucagon as a third molecular target in addition to GLP-1 and GIP?
As someone who has experimented with countless fat loss agents and weight loss drugs, from over-the-counter supplements to underground drugs, I KNOW there are so many targets worth pursuing.

(Source)
Why not revive the long-abandoned pursuit of leptin, the hormone that is known to downregulate during intense dieting, thereby increasing energy expenditure while making it far easier to inhibit food intake?
(NOTE: Unless something radically changes, people are no longer researching drugs to tackle leptin because its promise in human studies completely flopped… not to mention it simultaneously participates in the body’s response to a caloric deficit)
Or how about Neuropeptide Y (NPY), where blocking it may potentially lower insulin resistance and further contribute to lower food intake as well?
On a certain level, there HAD to be something uniquely worthwhile about glucagon to make it worthwhile!
One 2024 Diabetes, Obesity and Metabolism study gave me a helpful clue.
The study begins by talking about how the unimolecular GLP-1 receptor agonists (GLP-1RAs) such as Liraglutide and Semaglutide are known to induce side effects that lead to GLP-1RA discontinuation.
The most common ones by far are gastrointestinal in nature: Nausea, vomiting, diarrhea, and gastro-oesophageal reflux.
Based on prior animal studies showing a possible reduction in these side effects when a GLP-1RA was paired with a GIP receptor agonist, researchers wanted to see if the same thing would happen in humans:
“Participants were randomly assigned 1:1 using a randomization table to receive a single subcutaneous dose (day 1) of either LY (25 mg) or placebo (PBO) (comparable volume), with the alternative blinded treatment administered on day 1 of the second treatment period. The half-life of LY is approximately 11-14 days.6
For both treatment periods, this injection was followed by once-daily dosing of liraglutide, in a dose-escalation paradigm that increased daily from 0.6 mg subcutaneously (sc) (day 2) to 2.4 mg sc (day 5), followed by daily dosing at 2.4 mg through day 9. An 8-week washout period separated the two treatment periods in the crossover study.
Participants, investigators and clinic staff were blinded to LY versus PBO treatment assignment; only the clinic pharmacist was unblinded. Liraglutide was open label”

(LY = LY3537021, a GIP receptor agonist manufactured by Eli Lilly)
The test subjects were healthy males or females between the ages of 21 and 60 years old.
Here’s what the researchers found:

With the exception of diarrhea, there was a significant and uniform decrease in adverse events when Liraglutide was paired with LY3537021 compared to Liraglutide alone.
This observation coincides with my own personal experience, where Tirzepatide almost always leads to fewer side effects than Semaglutide.
Overwhelmingly, the same has been seen in people within my Fully Optimized Health community and my private inner circle.
And then I started asking myself more questions:
- Would targeting the glucagon receptor on top of the GLP-1 and GIP receptors lead to even fewer side effects?
- If no difference in side effect severity or frequency is noted, would you see better results with respect to weight loss, biomarker improvements, appetite suppression, and so on?
- Could you possibly see NEW outcomes like increased energy expenditure, direct lipolysis (fat burning), and skeletal muscle mass preservation?
This is the part where we take a deep dive into “triple agonist history”
What Happens When You Target GLP-1 And Glucagon?
While it is clear that both GLP-1 and GIP agonism are synergistic with respect to inducing weight loss and reduction of diabetes, I wasn’t sure if the same could be said of a GLP-1 + glucagon tag team.
Fortunately, this question was answered thanks to two Tweets I found.
The first was from a talk given at the annual ENDO meeting hosted by the Endocrine Society, specifically one from last year:
A 20 year collaborative journey developing retatrutide is coming to fruition.
Retatrutide which demonstrates 24.2% weight loss in its phase 2 trial is currently in Phase 3 trials for the treatment of obesity
Excellent talk on why #ChemistryMatters by Richard DiMarchi, PhD… pic.twitter.com/7eFnsYofRK
— Michael Weintraub, MD (@MWeintraubMD) June 2, 2024
I had a very hard time believing Retatrutide was nearly 2 decades in the making, especially given nobody I knew was even talking about the possibility of a triple receptor agonist peptide.
But the three studies featured in the tweet above gave me an idea of where to look.
Especially because it reminded me of a talk given at the ADA 83rd Scientific Sessions in 2023 titled “Why Three? Leveraging the Metabolic Action of Glucagon in Retatrutide, a Novel GIP/GLP-1/Glucagon Receptor Triagonist”:
So why glucagon agonism in a triple agonist? Impact on liver and weight. Slides below include details. #ADA2023 #obesity ⬇️ pic.twitter.com/Alxdoe27YV
— Abd Tahrani (@AbdTahrani) June 26, 2023
Sadly, I wasn’t able to get access to the video presentation or the full slide deck for either of the two talks.
Nevertheless, the 2009 study published in Nature Chemical Biology would hopefully give me the answers I’m seeking.
The excerpts from the study tell an interesting story:
“GLP-1R agonism safely improves glycemic control in people with adult-onset diabetes, with simultaneous reduction in body weight”
“Acute glucagon administration reduces food intake in animals and in humans, and some reports indicate that sustained glucagon receptor (GCGR) activation not only decreases food intake but also promotes lipolysis and weight loss. Chronic investigation of glucagon’s metabolic effects are challenging since the native hormone is rapidly degraded and has poor solubility and stability in physiological buffers”
Professor D’Alessio #ADA2023 highlights the early work of Stephen Bloom examining glucagon alone vs. Glucagon+GLP-1 in control of food intake and energy expenditure pic.twitter.com/cSlxGdsdER
— Daniel J Drucker (@DanielJDrucker) June 26, 2023
Yet at first glance of the existing literature, you would think this approach would be a dead end:
“… glucagon and GLP-1 have classically been thought to oppose each other in controlling blood glucose. Glucagon acts directly at the liver to raise blood glucose by stimulating gluconeogenesis and glycogenolysis, whereas GLP-1 acts by multiple mechanisms to lower glucose, most notably by enhancing glucose stimulated insulin synthesis and secretion at the pancreas”
But when you practice real science, real-world results don’t always match up with what “should” theoretically happen.
The researchers hypothesized that the effects of GLP-1 agonism would cancel out – if not minimize – any effects of glucagon agonism with respect to raising glucose levels and insulin secretion.
Furthermore, they also proposed the possibility of GLP-1’s induction of satiety working in tandem with glucagon’s lipolytic and thermogenic properties:
“A set of potent glucagon and GLP-1 co-agonists having differing activity at each receptor of interest was synthesized and biochemically characterized in vitro. Two specific glucagon analogs enhanced for sustained action and engineered to have activity at the GLP-1R comparable to that of native GLP-1 were studied pharmacologically in rodent obesity models.
Weekly administration of PEGylated peptides normalized adiposity and glucose tolerance in diet-induced obese mice. Body weight reduction was achieved by a loss of body fat resulting from decreased food intake and increased energy expenditure. The amount of body weight and fat loss increased with greater glucagon receptor agonism. These co-agonist compounds also normalized glucose and lipid metabolism and reduced liver steatosis”
The increased fat oxidation and inhibition of lipogenesis previously observed with glucagon infusions were also seen here.
But the last point about reducing liver steatosis (i.e. excess fat accumulation in liver cells) was important as it opens up the doors for targeting a new medical condition.
Which brings us to the 2013 paper featured in the one slide within the first Tweet I posted, titled “Unimolecular Dual Incretins Maximize Metabolic Benefits in Rodents, Monkeys, and Humans”.
What this study did was validate the idea of targeting both the GLP-1 and GIP receptors together with a single peptide molecule (as seen with the study shared in the prior section of this article).
After synthesizing a test candidate that uniformly targeted both receptors, here is what the researchers found:
“… demonstrated enhanced antihyperglycemic and insulinotropic efficacy relative to selective GLP-1 agonists. Notably, this superior efficacy translated across rodent models of obesity and diabetes, including db/db mice and ZDF rats, to primates (cynomolgus monkeys and humans).
Furthermore, this co-agonist exhibited synergism in reducing fat mass in obese rodents, whereas a selective GIP agonist demonstrated negligible weight-lowering efficacy. The unimolecular dual incretins corrected two causal mechanisms of diabesity, adiposity-induced insulin resistance and pancreatic insulin deficiency, more effectively than did selective mono-agonists.”
Additionally, modifying the test molecule to where less frequent administration was required led to fewer gastrointestinal side effects.
To recap:
- GLP-1 & GIP co-agonism, along with GLP-1 & glucagon co-agnoism, can lead to better reduction of insulin resistance AND fat mass compared to GLP-1 agonism alone
Logically, the next move would be to test GLP-1 & GIP & glucagon agonism simultaneously with one therapeutic peptide.
The only thing not known at this stage is whether all three receptors should be targeted equally, or if an uneven balance (targeting GLP-1 and GIP more that glucagon, for example) will provide the most optimal results possible.
This takes us to the 2015 paper featured in the ENDO 2024 talk, where this concept is put into action for the first time in history.
But before I get to that, I want to highlight a separate paper published in 2013 where the triple agonism concept was applied for the first time in mice.
Nine separate peptides were designed to be resistant to enzymatic cleavage (i.e. they are longer-lasting in the body), based around the amino acid sequences of GLP-1, GIP and glucagon.
After testing all nine peptides on obese diabetic mice, the peptide targeting all three receptors (referred to as “[dA2]GLP-1/GcG” in the study) was further examined:
“Acute administration of [dA2]GLP-1/GcG in combination with glucose significantly lowered plasma glucose and increased plasma insulin in normal and obese diabetic (ob/ob) mice. Furthermore, [dA2]GLP-1/GcG elicited a protracted glucose-lowering and insulinotropic effect in high fat-fed mice.
Twice daily administration of [dA2]GLP-1/GcG for 21 days decreased body weight and nonfasting plasma glucose and increased circulating plasma insulin concentrations in high fat-fed mice. Furthermore, [dA2]GLP-1/GcG significantly improved glucose tolerance and insulin sensitivity by day 21. Interestingly, locomotor activity was increased in [dA2]GLP-1/ GcG mice, without appreciable changes in aspects of metabolic rate.”
And there we have it — the proof-of-concept for a triple receptor agonist designed to help both diabetic and obese patients.
A very rare case in medicine and in health optimization where more is better!
The Triple Acting GLP-1, GIP And Glucagon Agonists Tested So Far

So what was the first triple GLP-1, GIP and glucagon (GGG) agonist fully tested with the intention of carrying it to the market as an FDA-approved pharmaceutical drug?
And where does Retatrutide fit in this short history of drug development?
I AM going to review them one at a time, showing you the scientific evidence for each one and where they currently are in the clinical pipeline.
MAR423, a.ka. NNC9204-1706 or NN9423 (Novo Nordisk)
It is here where we finally reach the first GGG agonist to evolve from a neat study into something seriously pursued at the clinical trial level.
And the 2015 paper mentioned near the end of the previous section: “A rationally designed monomeric peptide triagonist corrects obesity and diabetes in rodents”
Researchers first looked at male mice with diet-induced obesity and conducted several experiments involving mono-agonists, plus a GIP/GLP-1 co-agonist in combination with a glucagon agonist.
Overwhemingly, the combination approach (which targeted all 3 receptors) fared better compared to every other approach that targeted one or two receptors.
Not only was the greatest decrease in body weight observed, but the biggest reduction in blood glucose levels and cumulative food intake as well.
This gave the researchers enough reason to pursue the synthesis of the unimolecular tri-agonist MAR423, with the hopes of targeting all 3 receptors without any cross-reactivity or cancelling out of beneficial effects.
With additional testing, daily administration of MAR423 led to the greatest degree of improvement in metabolic benefits when compared to all other co-agonists and mono-agonists.
This was true across body weight change, fat mass change, fasted blood glucose levels, cholesterol levels, and higher plasma insulin levels.
To be more specific: MAR423 led to a 26.6% bodyweight reduction in 20 days, overshadowing the 15.7% observed with a GLP-1R/GIPR co-agonist approach.
And all of this was done without a significant loss of lean mass, or hypoglycemia (when blood sugar gets too low)… both in lean mice and in mice with diet-induced obesity.
But this study is especially important for two reasons…
One, it was a MASSIVE upgrade compared to the tri-agonist featured in the 2013 paper:
“In the most recent report, the total reported weight loss after three weeks of twice-daily administration was no more than 3% relative to vehicle control at a total dose of 50 nmol kg−1 d−1.
Our synthesis of these purported triagonists and subsequent in vitro analysis revealed these peptides to be dramatically reduced in potency relative to the native hormones (nearly 100-fold) and to our triagonist (nearly 1,000-fold).”
Two, the paper definitively demonstrated how the biological cascades induced by three peptide hormones – GLP-1, GIP, glucagon – can work synergistically when activated with a single tri-agonist:
“We demonstrate that these individual constituent activities harmonize to govern the overall metabolic efficacy, which predominantly results from synergistic glucagon action to increase energy expenditure, GLP-1 action to reduce caloric intake and improve glucose control, and GIP action to potentiate the incretin effect and buffer against the diabetogenic effect of inherent glucagon activity.
These preclinical studies suggest that, so far, this unimolecular, polypharmaceutical strategy has potential to be the most effective pharmacological approach to reversing obesity and related metabolic disorders.”
A follow-up study in 2017 attempted to replicate these results, except this time they used FEMALE mice.
Why does this matter?
It seems that female mice, for some reason, have a higher degree of intolerance to glucose and a greater resistance to diet-induced obesity compared to mice.
On top of that, women react differently to weight loss drugs than men do with respect to higher rates of side effects and different weight loss outcomes.
(It would be too complicated to explain WHY this is the case, although you can easily chalk this up to a woman’s hormonal system and menstrual cycle leading to greater variations on the observed effects of a weight loss drug)
Fortunately, after 27 days of daily subcutaneous injections of either MAR423 or placebo, there was enough evidence to suggest women would benefit just as much as men from the triple GGG approach:
“[MAR423] inhibits food intake and decreases body weight and body fat mass with comparable potency in male and female mice that have been matched for body fat mass. Treatment improved dyslipidemia in both sexes and reversed diet-induced steatohepatitis to a larger extent in female mice compared to male mice.
Conclusions: We herein show that a recently developed unimolecular peptide triagonist is equally efficient in both sexes, suggesting that this polypharmaceutical strategy might be a relevant alternative to bariatric surgery for the treatment of obesity and related metabolic disorders.”
Another study published earlier in 2017 looked at the effect of MAR423 on cognitive behaviors in mice with Alzheimer’s Disease.
This is relevant given Type 2 Diabetes increases your risk for contracting numerous other diseases, with Alzheimer’s being one of them.
Unfortunately, the entire study is written in Chinese and all I could find was the abstract in English.
So I’ll cut and paste the most important finding here:
“…chronic treatment with the Triagonist (i.p.) significantly reversed the impairments in working memory of 3xTg-AD mice, with an obvious increase in the percentage of correct spontaneous alternation in the Y maze; the Triagonist treatment also improved long-term spatial memory and re-learning ability of 3xTg-AD mice in classical Morris water maze and reverse water maze tests, with decreased escape latency in under water platform tests and increased swimming time in probe tests.
ELISA and Western blot experiments showed that the Triagonist up-regulated the levels of cAMP, PKA and p-CREB in the hippocampus of 3xTg-AD mice.
These results indicate that GLP-1/GIP/Gcg receptor Triagonist can improve the cognitive behaviors in 3xTg-AD mice, and the up-regulation of hippocampal cAMP/PKA/CREB signal pathway may mediate the neuroprotection of the Triagonist, suggesting that the GLP-1/GIP/Gcg receptor Triagonist may be a novel therapeutic strategy for the treatment of AD”
Two more mouse studies published in 2018 (here and here) expanded on this concept of treating Alzheimer’s disease, noting some additional benefits.
There was the reduction in damage done to the hippocampus, decreased neuroinflammation, along with a possible neuroprotective effect via neurogenesis and upregulation of BDNF.
The last pre-clinical study on MAR423, released in 2020, didn’t reveal much more than what was already known in the context of treating Alzheimer’s Disease.
While there were some specifics about increased memory formation, neuronal excitability, and synaptic transmission, nothing significant was found in the context of the other papers.
The only references to any clinical studies done are two Phase 1 trials, one assessing safety through ascending doses, and another using a fixed dose.
Both of them are completed… but there aren’t any publications or press releases outlining the results.
This drug is effectively discontinued and it is unclear why, although I AM suspecting the once-daily subcutaneous injections would prove to be unfavorable.
Especially given that agents like Semaglutide and Tirzepatide were already succeeding with once-weekly injections.
(Allegedly, Novo Nordisk has gone back to the drawing board in order to create a once-weekly injectable tri-agonist GGG peptide)
In general: Less frequent injections lead to greater patient adherence, and a pill is almost always favorable to an injection.
DA2GIP-Oxm
Although I AM cheating a little here, this never-to-be-heard-of-again tri-agonist only has a single paper dedicated to its name.
It was created by taking Oxyntomodulin, a 37-amino-acid long peptide hormone that naturally occurs within the colon, and making a slight modification to it.
On its own, Oxyntomodulin targets the GLP-1 and glucagon receptors simultaneously.
This suggests, as we’ve seen earlier in this article, that it can enhance both insulin secretion and energy expenditure while decreasing caloric intake.
The modification involved adding a “D-Alanine-GIP” moiety to the N-terminal so the newly formed DA2GIP-Oxm would also target GIP at the same time.
When DA2GIP-Oxm was given once daily to obese-diabetic mice fed a high-fat diet, the results look promising at first:
“Once-daily administration of DA2GIP-Oxm for 15 days in HFF mice lowered body weight (13% reduction), reduced plasma glucose (40% reduction) and increased plasma insulin (1.7-fold increase). Furthermore, glycemic responses were improved (38% reduction) and glucose-mediated plasma insulin concentrations enhanced (2-fold increase). These improvements in metabolic control were independent of changes in food intake and insulin sensitivity”
However, a review paper released 5 years later summarizes why DA2GIP-Oxm remained an idea destined to be forgotten:
“…it was less potent at each receptor (GIPR, GLP-1R, and GCGR) compared with the respective native ligand.
DA2GIP-Oxm more potently reduced glycemia and decreased body weight compared with any individual peptide; however, it is important to note that comparison with the clinical standard, liraglutide, was not performed and, based on percentage weight loss, would have performed similarly.”
XFL6
This is another obscure triple receptor agonist included for completion’s sake, but it’s nothing worth your time.
The diagram I took from the study below, which involved mice with diet-induced obesity, will show you why:
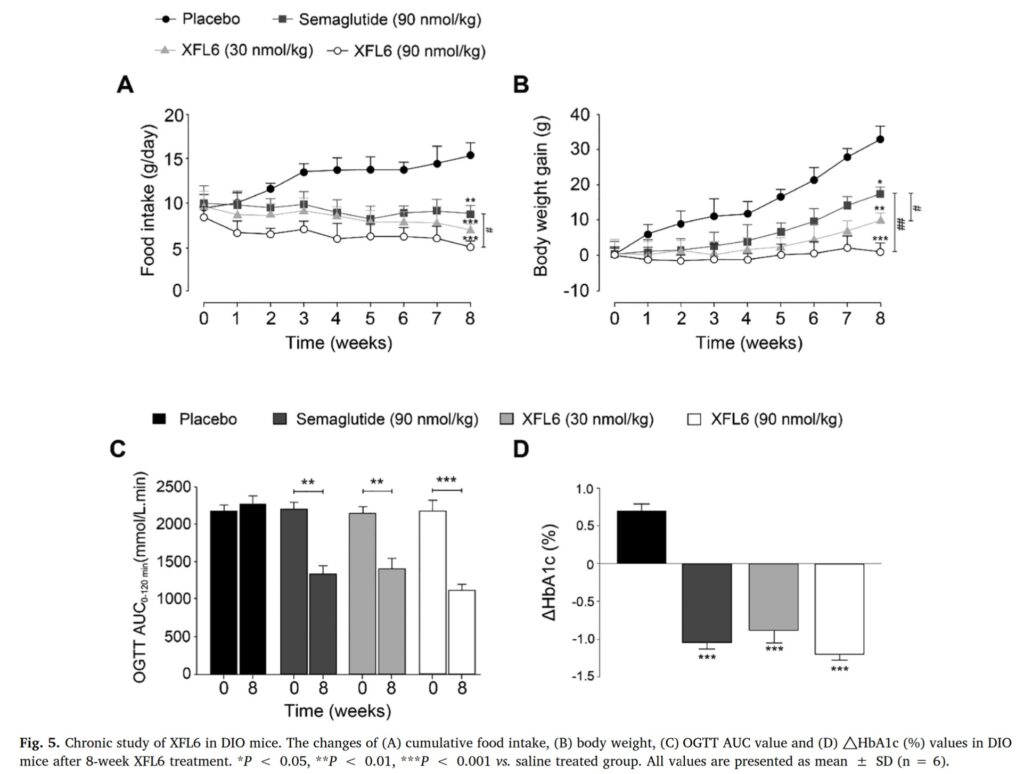
Even though food intake went down significantly and there’s a noticeable decrease in blood glucose, the BEST bodyweight outcome involved weight staying the same after 8 weeks of daily administration of XFL6 at the highest dose.
Moving on!
HM15211, a.k.a. Efocipegtrutide (Hanmi Pharmaceutical)
Based on what I’ve seen thus far, it doesn’t appear this molecule will be outcompeting Retatrutide anytime soon.
And I’ll tell you why.
First, it seems the drug will primarily be targeted towards people with fatty livers.
If you take a look at their poster presentation in 2020 summarizing the results of their Phase 1b/2a clinical trial, the weight loss results aren’t too impressive:
“The mean (SD) relative changes from baseline in liver fat at week 8 were −14.9 (12.2) % for 0.01 mg/kg ( p = 0.13), −43 (23.5) % for 0.02 mg/kg (p < 0.0001), −44.5 (46.6) for 0.04 mg/kg ( p = 0.0005), −71 (23.8) % for 0.06 mg/kg ( p < 0.0001), −80.3 (13.2) % for 0.08 mg/ kg ( p < 0.0001), vs. −1.2 (24.5) % for placebo group.
The mean (SD) relative changes from baseline in liver fat at week 12 were −19.6 (12.2) % for 0.01 mg/kg ( p = 0.30), −36 (28.1) % for 0.02 mg/kg ( p = 0.06), −38 (53.5) % for 0.04 mg/kg ( p = 0.12), −59.3 (27.6) % for 0.06 mg/kg ( p = 0.0020), and −5.7 (37.8) % for placebo group. The liver fat reduction proportionally increased by escalating doses and the observed maximum liver fat reduction at week 12 was 88% by currently available data.
HM15211 decreased body weight compared with placebo across all treatment groups. Placebo-corrected kg and % reduction of body weight were −1.3, −1.8*, −2.1*, −3.1*, and −4.3* kg (−1.2, −1.9*, −2.2*, −2.9*, and −4.4*%) at week 8 and −2.1, −3.1*, −1.9, −4*, and −5.3* kg (−1.9, −3.4*, −2.1, −3.8*, and −5.1* %) at week 12 in 0.01 to 0.08 mg/kg dose cohorts, respectively (*p < 0.05).
HM15211 was shown to be well tolerated. The most common dose-dependent adverse events were mild gastrointestinal symptoms. Two subjects at different dosing cohorts developed hyperglycemia, but rapidly resolved with IP discontinuation”
Granted, a ~5% loss of your body weight at 12 weeks (using the highest dose of HM15211) could POTENTIALLY expand to 20% after 48 weeks, which is similar to the numbers Retatrutide put up at its highest dose.
But we have no idea if weight loss will continue to be linear after the 12-week mark, or plateau and not go down much further.
At the same time, the reduction in liver fat was quite impressive and I suspect this is the angle they’ll be pushing.
In other words… while Retatrutide will be reserved for the ultra-fat people who want to get to a healthy weight ASAP and the bodybuilders who want to make getting shredded a breeze, HM15211 will be for the inflamed dumpster fires that additionally have liver problems.
According to the official Hanmi Pharmaceutical website, the goals for this compound are as follows:
“Maximal efficacy for liver fat removal by three combined mode of action (energy intake, β-oxidation, and de novo lipogenesis)
Maximal efficacy for Improvement of liver inflammation by multiple incretin action in cooperation with favorable liver targeting
Direct down-regulation of hepatic stellate cell activation”
Considering they’ve discontinued pursuing the drug for other purposes such as Alzheimer’s, obesity, and Type 2 Diabetes, it’s all-in or face abandoning a years-long project to get HM15211 to market .
That webpage also has several links to presentations of clinical work the company has done for HM15211, such as its anti-inflammatory and anti-fibrotic properties, and ability to combat liver fibrosis.
Currently, Hamni Pharmaceutical is conducting a Phase 2b clinical trial in Korea and the US for patients with NASH (Non-alcoholic steatohepatitis) (NASH), the most severe type of non-alcoholic fatty liver disease (NAFLD).
The study design for this trial can be found in a Contemporary Clinical Trials paper published in 2023.

SAR441255 (Sanofi)
The timeline on this particular tri-agonist is a bit weird, so stay with me.
The earliest mention of SAR441255 I found dates back to 2019, when Sanofi mysteriously announced the discontinuation of further efforts to get it to market while it was in Phase 1 clinical trials for diabetes/obesity.
Whether it was due to a change in strategy or some other internal reason, we will never know exactly why it was shelved.
And regrettably, it was only being studied for obesity and type 2 diabetes… so no chance of SAR441255 ever getting resurrected.
But out of nowhere, it gets this MASSIVE paper published in Cell Metabolism in 2022.
This is a seriously legitimate journal that ranks all the way up there with Nature, where you don’t get your findings published unless they truly mean something.
The study contains the results of not only in vivo studies and an animal study, but the results of the Phase 1 clinical trial that got shut down.
Here’s the summary, according to the abstract:
“SAR441255 displays high potency with balanced activation of all three target receptors. In animal models, metabolic outcomes were superior to results with a dual GLP-1/GCG receptor agonist.
Preclinical in vivo positron emission tomography imaging demonstrated SAR441255 binding to GLP-1 and GCG receptors.
In healthy subjects, SAR441255 improved glycemic control during a mixed-meal tolerance test and impacted biomarkers for GCG and GIP receptor activation. Single doses of SAR441255 were well tolerated.
The results demonstrate that integrating GIP activity into dual GLP-1 and GCG receptor agonism provides improved effects on weight loss and glycemic control while buffering the diabetogenic risk of chronic GCG receptor agonism.”

(Source)
Within the animal model involving diabetic monkeys with obesity), superior weight loss was observed with SAR441255 compared to a dual GLP-1R/GCGR agonist but similar results were achieved for glucose control.
And in the mouse model, SAR441255 was only superior to the dual GLP-1R/GCGR agonist once researchers cranked the twice-daily dose to the highest level possible.
As for the Phase 1 clinical study (NCT04521738), it was a single-dose subcutaneous injection to assess how safe SAR441255 was at varying doses (3, 9, 20, 40, 80, or 150 ug) in patients ranging from lean to overweight.
Surprisingly, SAR441255 had a short half-life ranging from ~3-6 hours and reached maximum concentration in the blood within 3 hours following administration.
Even more interesting was how blood glucose levels returned back to normal 1-2 hours after the injection.
SIde effects were mild, took place 3-4 hours following the injection, and were the usual list of gastrointestinal adverse events reported with GLP-1 peptides in general (dry mouth, nausea, vomiting)
Sadly, due to the small nature of the study and the few participants eligible to participate, researchers were unable to determine SAR41255’s effects on energy expenditure or food consumption.
Conclusion: So How Good Can Retatrutide REALLY Be?

I was initially surprised to see that Retatrutide is the only triple GGG peptide currently succeeding in clinical trials, without any sign of dropping out whatsoever.
It didn’t make much sense to see several companies spend the last decade attempting to make their own tri-agonist drug candidate, complete all preclinical research, maybe reach Phase 1/2 clinical trials in an instance or two, and then disappear.
Was there something these companies found they didn’t want the public knowing?
Is it something perhaps Eli Lilly, the makers of Retatrutide, did a better job of concealing from the watchful eye of the public?
I AM doubtful the once-daily administration was the straw that broke the camel’s back.
Either way… in Part 2, you’re going to discover why Retatrutide is far more than a one-hit wonder in the anti-obesity drug sector.
With all the boring stuff now covered, it’s time to get into what makes it an unbeatable powerhouse with unparalleled potential to reverse obesity once and for all.
Stay tuned for its release!
Check out this brand new video from Hunter Williams and I discussing everything you desire to know when using Retatrutide in 2025 and beyond.
And if you want to get ahead of Part 2 by stocking up on Retatrutide for yourself, then listen closely:
BioLongevity Labs sets the benchmark for USA-manufactured research peptides, with a relentless focus on purity, stringent third-party testing, and top-notch customer service.
We consistently deliver the highest quality products, trusted by professionals for both personal and clinical use.
Whether you’re looking to elevate your performance or integrate these products into research applications, BioLongevity Labs is THE most trusted source you can count on.
Use code JayC to get 15% off your order!
When you’re ready to take your Retatrutide journey to the next level, I invite you to join my Fully Optimized Health Private Membership Group.
You’ll get exclusive access to cutting-edge protocols, expert insights, and a community of high-performers committed to living their best lives.
As always:
Raise Your Vibration To Optimize Your Love Creation!
Now, if you want to take your health optimization journey to the next level…
You’ll have to dive deeper into using peptides to optimize health, especially if you’re in your 30s and beyond.
And in doing so, you’ll unlock cutting-edge biohacking intel and the latest and greatest in elite health optimization strategies.
If that sounds like you, don’t forget to check out our other premium educational content dedicated to helping you fully optimize your health:
Peptides Demystified – the step-by-step, A-to-Z system for newbies desiring to master peptide use for the first time and forever.
The Ultimate GLP-1 Video Masterclass – how to PROPERLY utilize the world’s most powerful weight loss drugs for enhanced fat loss and overall longevity.
The Modern Woman’s Peptide Course – a must-have resource for any woman seeking to become more feminine, sexier, leaner, and healthier through the use of peptides.
Life Enhanced – Unlock the secrets to TOTAL Mind-Body-Spirit Optimization as Hunter Williams and I teach you how to live at the tip of the spear.
30 Days 2 Shredz – Reprogram Your Mind and Body for Maximum Fat Loss in Minimum Time with our Optimized Fasting Protocol
See you on the inside!


