Written by Jay Campbell
Written by Jay Campbell



Retatrutide (LY3437943) is blowing up both the pharmaceutical world and the bodybuilding world for the same reason:
This “triple G” multi-receptor agonist manufactured by pharmaceutical company Eli Lilly has paved the way for what could be an entirely new generation of anti-obesity drugs.
It is unquestionably in first place within the current race among Big Pharma companies to have the best-selling weight loss medication of all time.
For the first time in modern medical history, we FINALLY have the pharmacological means to effectively and safely treat obesity (and the many conditions that result from it) by target multiple biological pathways at once.
The only things standing in its way of making history are its ongoing Phase 3 trials, the coveted stamp of approval from the FDA, and possibly upcoming competitors in the clinical pipeline.
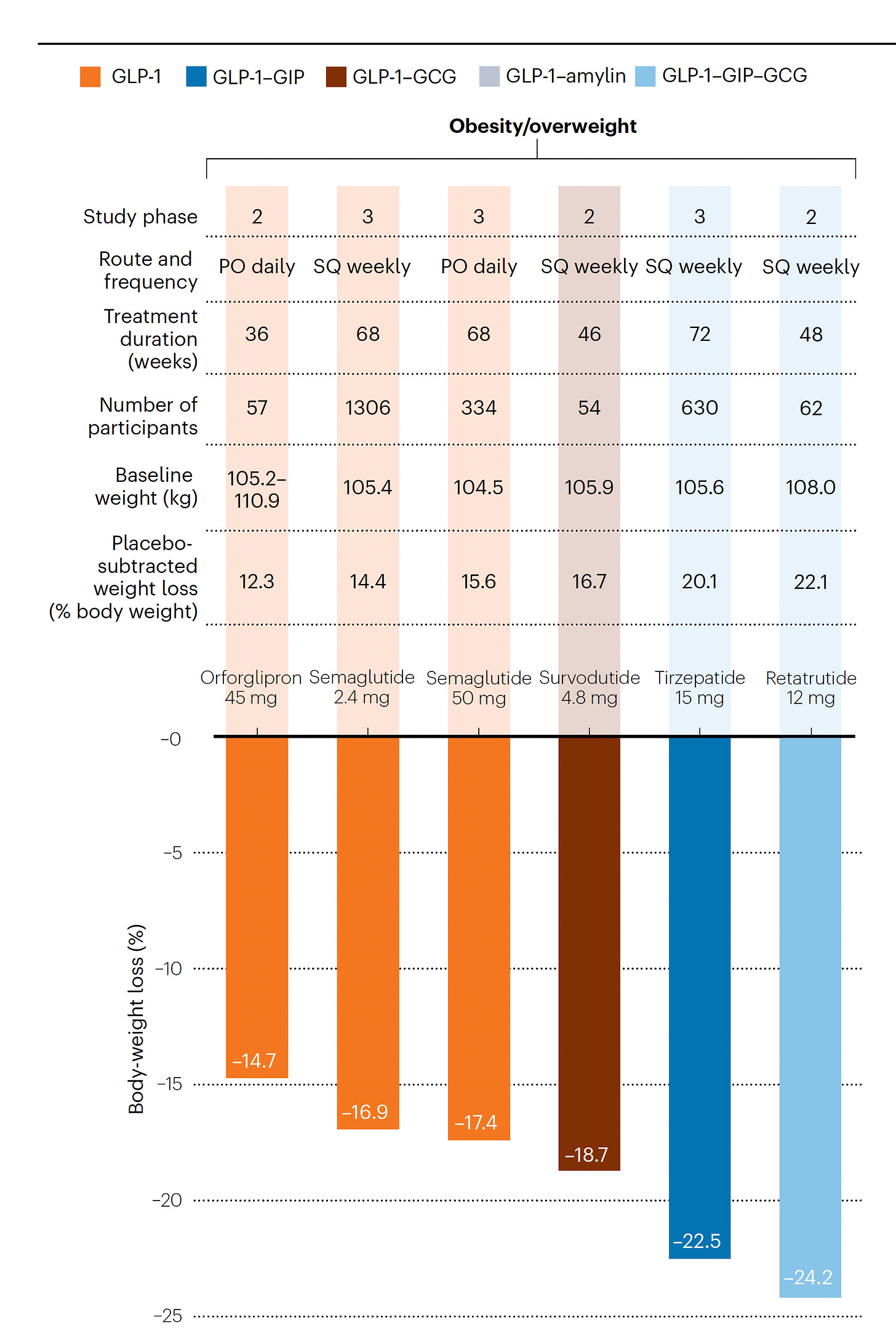
First came Ozempic, then came Tirzepatide, and now Retatrutide holds the throne as the world’s most powerful fat loss drug.
In Part 1, we talked about the history of triple receptor hormone agonists targeting GLP-1, GIP, and glucagon.
In this second installment, we will dive into the health benefits of Retatrutide and its practical applications.
Reviewing Retatrutide’s Mechanism Of Action

(Source)
As elucidated in Part 1, Retatrutide works by targeting the receptor of three peptide hormones in the human body.
GLP-1 (Glucagon-Like Peptide-1)
- Delayed gastric emptying (lowers appetite and promotes extended satiation)
- Increased secretion of insulin
- Lowered glucose levels
GIP (Glucose-dependent Insulinotropic Polypeptide)
- Increased uptake and storage of glucose
- Elevated fatty acid uptake
- Increased secretion of insulin
GCG (Glucagon)
- Elevated lipolysis and energy expenditure
- Increased secretion of insulin
- Promotion of satiety (feeling full)
Prior work on developing triple receptor agonist molecules shows a synergistic effect between GLP-1, GIP and GCG when said molecule is optimized to adequately target their respective receptors.
Further optimization led to once-weekly administration instead of daily administration, longer-lasting presence in plasma (blood), superior target outcomes (i.e. weight loss), and minimization of side effects.
The real struggle up to this date hasn’t been the increased weight loss that results, but rather replicating this finding from animal studies in the human population.
As of right now, Retatrutide is the only viable tri-agonist with serious potential to reach market availability.
This takes us to the current body of clinical evidence investigating this experimental drug candidate.
Human Clinical Trials Investigating Retatrutide

As of this writing, there are only four studies where Retatrutide has been examined for its effects in patients who are diagnosed with obesity and/or Type 2 diabetes.
Yet they provide a plethora of data to observe its long-term safety and efficacy in its intended population.
We can also reasonably infer how Retatrutide can possibly benefit healthy and lean adults seeking dramatic changes in body composition.
Phase 1B – Type 2 Diabetes (NCT04143802)
This was a randomized, double-blind and placebo-controlled trial designed to examine the safety profile of Retatrutide via doses that gradually increase over the duration of the study.
Test Subjects (n = 72):
- Average age of the subjects was 20-70 years old
- Diagnosed with type 2 diabetes for at least 3 months prior to enrollment
- No glucose-lowering medications were allowed within 3 months before the trial started (except for Metformin, in which case the dose had to be unchanged)
- Body mass index (BMI) of 23-50 kg/m², with bodyweight remaining stable (<5% change) within 3 months prior to the trial starting
- Haemoglobin A1c (HbA1c) value of 7.0–10.5%
Dosing Schedule:
- Patients were assigned to seven separate treatment routes for 12 weeks
- Route #1 = Placebo
- Route #2 = 1.5mg Dulaglutide
- Route #3 = 0.5mg Retatrutide injected subcutaneously once a week
- Route #4 = 1.5mg Retatrutide injected subcutaneously once a week
- Route #5 = 3.0mg Retatrutide injected subcutaneously once a week
- Route #6 = 3.0mg Retatrutide injected subcutaneously once a week for 4 weeks, then 6mg for 8 weeks (3/6)
- Route #7 = 3.0mg Retatrutide injected subcutaneously once a week for 2 weeks, then 6mg for 2 weeks, then 9mg for 4 weeks, then 12mg for 4 weeks (3/6/9/12)
- Randomization was done in the following manner per cohort: at least 9 people receive Retatrutide, 3 people receive the placebo, 1 person receives dulaglutide
Clinical Outcomes:

- Placebo-adjusted mean changes in bodyweight (kg)
- Dose-dependent reductions were observed
- Dulaglutide, 1.5mg: 0.08
- Retatrutide, 3mg: -4.71
- Retatrutide, 3mg/6mg/9mg/12mg: -8.96
- Placebo-adjusted mean changes in waist circumference (cm)
- Dose-dependent reductions were observed
- Dulaglutide, 1.5mg: -2.6
- Retatrutide, 3mg: -5.1
- Retatrutide, 3mg/6mg/9mg/12mg: -6.4
- Placebo-adjusted mean changes in plasma glucose (mmol/L)
- Dose-dependent reductions were observed
- Dulaglutide, 1.5mg: -2.4
- Retatrutide, 3mg: -2.8
- Retatrutide, 3mg/6mg/9mg/12mg: -2.9
- Placebo-adjusted increases in appetite reduction and satiety scores from baseline
- Statistically significant for the 3mg/6mg Retatrutide group, but not the 3mg/6mg/9mg/12mg Retatrutide group
- Placebo-adjusted decreases in serum lipid parameters
- LDL cholesterol: As large as a 31% reduction, observed in the 3mg/6mg/9mg/12mg Retatrutide group (+47% for Dulaglutide 1.5mg)
- VLDL cholesterol: -34.2% observed in the 3mg/6mg/9mg/12mg Retatrutide group
- Triglycerides: Dose-dependent, and as large as a 44% reduction observed in the 3mg/6mg/9mg/12mg Retatrutide group
- Mean diastolic/systolic blood pressure
- Up to 12 mm Hg reduction for systolic blood pressure observed with Retatrutide (3mg/6mg/9mg/12mg)
- Up to 2 mm Hg reduction for diastolic blood pressure observed with Retatrutide (3mg/6mg/9mg/12mg)
- Heart rate
- An increase between 2-13 BPM (beats per minute) in the three highest-dosed Retatrutide groups 24 hours after the last treatment dose (-1 to 10 BPM when averaged over the last 4 weeks of treatment)
- No significant differences in major cardiovascular events such as tachyarrhythmias (abnormal heart rate)
- Longer-term studies are required to assess whether early changes in heart rate seen with Retatrutide will diminish over time (and whether any detrimental effects result
Side Effects:

- Treatment-emergent adverse events (TEAEs) reported by 33 (63%) patients receiving Retatrutide, and 8 (54%) patients receiving placebo
- 4 patients (6%) discontinued treatment due to a TEAE, two of which were attributed to Retatrutide
- The most frequently reported TEAEs were gastrointestinal in nature, with diarrhea, nausea and abdominal distention being most common among the higher-dosed Retatrutide groups (relative to the lower-dosed groups)
- Any TEAEs related to pancreatitis, thyroid malignancies, and severe gastrointestinal events were reported
- Gastrointestinal TEAEs resolved within 10 days of onset, and were mild/moderate in nature
To conclude:
- Safety and tolerability for Retatrutide were acceptable, and comparable to other incretin receptor targeting agonists
- Once-weekly dosing of Retatrutide would be suitable
- Future studies should directly measure body composition and energy expenditure
- Ideally, Retatrutide should be compared head-on against agents such as Tirzepatide

(Source)
Phase 2 – Obesity (NCT04881760)
This was a randomized, double-blind and placebo-controlled trial designed to further examine Retatrutide’s safety and effectiveness in obese patients, both at single doses and escalating doses.
(Yes, this was the same study revealed at the American Diabetes Association’s 83rd Scientific Sessions in 2023 that got a LOT of media attention!)
Test Subjects (n = 338):
- Average age of the subjects was 18-75 years old
- Equal number of men and women were enrolled
- Subjects were obese (30-50 kg/m² BMI) or overweight (27-30 kg/m² BMI) with a minimum of one obesity-related condition (ex. hypertension)
- Patients with diabetes, had received or will receive surgery to treat obesity, and/or using a weight gain/loss medication changing body weight by +/- 5% within 3 months before screening, were excluded
Dosing Schedule:
- Patients were assigned to the following groups for 48 weeks in a 2:1:1:1:1:2:2 ratio, followed by a safety follow-up period of 4 weeks
- Group #1 = 1.0mg Retatrutide injected subcutaneously once a week
- Group #2 = 2.0 mg Retatritude injected subcutaneously once a week going to 4.0mg (gradual escalation of dose every 4 weeks for up to 12 weeks)
- Group #3 = 4.0 mg Retatritude injected subcutaneously once a week
- Group #4 = 2.0 mg Retatritude injected subcutaneously once a week going to 8.0mg (gradual escalation of dose every 4 weeks for up to 12 weeks)
- Group #5 = 4.0 mg Retatritude injected subcutaneously once a week going to 8.0mg (gradual escalation of dose every 4 weeks for up to 12 weeks)
- Group #6 = 2.0 mg Retatritude injected subcutaneously once a week going to 12.0mg (gradual escalation of dose every 4 weeks for up to 12 weeks)
- Group #7 = Placebo
But here’s where things get interesting, according to the procedures of the study:
“All the participants received a lifestyle intervention, including regular counseling sessions that were delivered by a dietitian or qualified health care professional and were based on U.S. government guidelines for a healthy diet and physical activity. The protocol did not require a specific energy deficit for the diet.”
Even in the supplementary information, specific details about diet and physical activity were missing.
Within a perfect world, calorie intake and physical activity (weightlifting, cardio, etc.) would have been precisely measured to rule out any underreporting of energy intake and/or over-reporting of energy expenditure.
Clinical Outcomes:

- Least-square mean percentage changes in bodyweight
- Placebo: -1.6% at 24 weeks, -2.1% at 48 weeks (-1.8kg)
- Retatrutide, 1mg: -7.2% at 24 weeks, -8.7% at 48 weeks (-9.4kg)
- Retatrutide, 4mg: -13.9% at 24 weeks, -17.8% at 48 weeks (-19.1kg)
- Retatrutide, 12mg: -17.5% at 24 weeks, -24.2% at 48 weeks (-26.2kg)
- Percentage of patients who reached weight reduction targets relative to baseline
- Placebo: 27 (≥5%), 5 (≥10%), 2 (≥15%)
- Retatrutide, 1mg: 64 (≥5%), 27 (≥10%), 16 (≥15%)
- Retatrutide, 4mg: 87 (≥5%), 73 (≥10%), 55 (≥15%)
- Retatrutide, 12mg: 100 (≥5%), 93 (≥10%), 83 (≥15%)
- Least-square mean percentage changes in waist circumference from baseline (cm)
- Placebo: -2.6
- Retatrutide, 1mg: -6.5
- Retatrutide, 4mg: -14.9
- Retatrutide, 12mg: -19.6
There were also some interesting observations about Retatrutide’s disproportionate impact on two subgroups:

Women lost more weight than men (28.5% vs 21.9% in the Retatrutide 12mg group), and people with a starting BMI of 35 or greater lost more weight than people with a starting BMI below 35 (26.5% vs. 22.1% in the Retatrutide group).
Although these findings are in line with existing studies looking at obesity drugs, the reason why here is not exactly clear: Hormonal profile, distribution of fat tissue, and differing body composition could all be potential factors.
Which brings me to one major limitation of this study… the lack of body composition data (i.e. how much of the weight loss was muscle, fat, glycogen, water, etc.).
This data will be the ultimate deterrent in showing how well these drugs preserve skeletal muscle mass with (and without) protective measures such as high protein intake and resistance training.
But let’s move on to the real reason why people can’t stop talking about this study.
The highest dose of Retatrutide (12mg) is what blew away all other weight loss medications currently in existence: Not only did everyone in that group lose at least 5% of their total bodyweight, but 1 out of every 4 patients lost 30% or more of their starting weight!
(Source)
And researchers mentioned in the discussion, this rate of weight loss is directly comparable what is observed with bariatric surgery!
For context… in one retrospective study tracking weight changes in 1787 American veterans for 10 years following Roux-en-Y gastric bypass (RYGB), they lost an estimated 31% of their starting bodyweight within the first year post-surgery.
It gets even better because the researchers have said the weight loss did NOT reach a plateau at the study cutoff, meaning even more weight loss would have been possible if the treatment period was extended.
I should also note there were some improvements in cardiometabolic risk factors that unfortunately didn’t get their own pretty diagram:
- 72% of patients in the Retatrutide groups who were prediabetic ended up normalizing their glycated hemoglobin levels (compared to 22% of patients in the placebo group)
- At least one anti-hypertensive medication was discontinued in the Retatritude 8mg group (41% of patients) and Retatrutide 12mg group (30% of patients)
- Significant reductions in systolic & diastolic blood pressure, fasting glucose, insulin, and all lipids (ex. triglycerides, LDL, total cholesterol) except HDL were observed within the Retatrutide groups at the 48-week mark.
Side Effects:
- 6-16% of the patients in the Retatrutide groups discontinued treatment due to adverse events (0% for the placebo group)
- 70% of patients receiving placebo reported at least one adverse event during the 48-week treatment period, whereas that number was 73-94% for patients receiving Retatrutide
- Gastrointestinal side effects were the most commonly reported, and happened most frequently in the Retatrutide groups (constipation, vomiting, nausea, diarrhea)
- Higher doses of Retatrutide led to more frequent side effects (particularly the 8mg and 12mg groups) and were somewhat reduced by starting at a lower dose
- Most of these side effects happened while the doses were increased
- Most of the side effects were mild or moderate
Overall, these observations were expected given what has been previously observed with other GLP-1 and GLP-1/GIP receptor agonists.
One particular side effect that caused a lot of alarm on social media was the heart rate increases observed in the Retatrutide groups, which were very clearly linked to dose escalations:

Within the Retatrutide groups, a total of 17 people reported abnormal heart rhythms (vs. 2 in the placebo group).
However, it should be noted these heart rate increases peaked at the 24-week mark and then started to normalize over time.
For this reason, researchers are suggesting patients with existing heart problems and severe gastrointestinal issues may not benefit from using Retatrutide.
Phase 2 – Diabetes (NCT04867785)
This was a randomized, double-blind and placebo-controlled trial designed to expand upon the Phase 1B study and determine Retatrutide’s safety and effectiveness across several dosing regimens in Type 2 diabetics.
(Like the prior clinical trial, its data was also released at the American Diabetes Association’s 83rd Scientific Sessions in 2023)
Test Subjects (n = 281):
- Average age of the subjects was 18-75 years old
- BMI = 25-50 kg/m²
- HbA1c = 7.0-10.5%
- 3 months prior to screening must have (a) been using >1000mg of Metformin daily or (b) undergone a diet and exercise treatment alone
- Bodyweight had to be within +/- 5kg for 3 months prior to randomization
Dosing Schedule:
- Patients were randomly assigned to the following groups for 36 weeks in a 2:2:2:1:1:1:1:2 ratio, followed by a safety follow-up period of 4 weeks
- Group #1 = Placebo
- Group #2 = 1.5mg Dulaglutide injected subcutaneously once a week
- Group #3 = 0.5mg Retatrutide injected subcutaneously once a week
- Group #4 = 2mg Retatrutide injected subcutaneously once a week, with dose escalation to 4mg
- Group #5 = 4mg Retatrutide injected subcutaneously once a week
- Group #6 = 2mg Retatrutide injected subcutaneously once a week, with dose escalation to 8mg
- Group #7 = 4mg Retatrutide injected subcutaneously once a week, with dose escalation to 8mg
- Group #8 = 2mg Retatrutide injected subcutaneously once a week, with dose escalation to 12mg
- Retatrutide dose was increased every 4 weeks where applicable (i.e. 2mg, 4mg, 8mg, 12mg) until maintenance dose was reached
Clinical Outcomes:

- Change in bodyweight from baseline after 36 weeks (%)
- Placebo = -3.28%
- 1.5mg Dulaglutide = -1.97%
- 4mg Retatrutide = -10.37% (-7.09% vs. placebo, -8.4% vs. Dulaglutide)
- 12mg Retatrutide (escalation) = -17.18% (-13.91 vs. placebo, -15.22% vs. Dulaglutide)
- Change in HbA1c from baseline after 36 weeks (mmol/L)
- Placebo = -3.32
- 1.5mg Dulaglutide = -14.86
- 4mg Retatrutide = -16.42 (-13.09 vs. placebo, -1.55 vs. Dulaglutide)
- 12mg Retatrutide (escalation) = -23.59 (-20.26 vs. placebo, -8.72 vs. Dulaglutide)
- Change in fasting insulin from baseline after 36 weeks (%)
- Placebo = -22.17%
- 1.5mg Dulaglutide = 35.86%
- 4mg Retatrutide = -20.42% (2.26% vs. placebo, -41.35 vs. Dulaglutide)
- 12mg Retatrutide (escalation) = -36.33% (-18.19% vs. placebo, -53.07% vs. Dulaglutide)
With respect to the primary endpoint of HbA1c, 27% of people in the 12mg escalation group achieved a reading of less than 5.7%, indicating normoglycaemia (normalized blood sugar levels) had been reached (19% for the 4mg group and 3% for both placebo and Dulaglutide groups).
Significant and clinically meaningful dose-dependent HbA1c reductions were specifically observed in patients taking 4mg-12mg of Retatrutide, and the same held true for weight loss.
To be more exact:
- Similar to the Phase 2 trial for obesity, the weight loss did not plateau and could have been far greater in the Retatrutide groups if the trial was allowed to continue
- Given that Type 2 diabetics are known to lose less weight than obese people without diabetes, the bodyweight changes seen in this study are to be expected.
Side Effects:

- There were no serious incidents of hypoglycaemia (too little blood sugar) reported, nor were there any maglinancies in the thyroid gland or reports persistent hyperglycaemia (too much blood sugar)
- 8% of patients across all Retatrutide groups collectively did not continue treatment because of an adverse event
- The most commonly reported adverse events in people taking Retatrutide were gastrointestinal in nature (constipation, diarrhea, vomiting, nasuea), were mild to moderate in severity, and happened more often in people taking larger doses of Retatrutide
All in all, patients on Retatrutide experienced a dramatic improvement in insulin sensitivity and any observed side effects were not significantly different in severity, type or frequency compared to the Phase 2 trial for obesity.
Phase 2 – Non-Alcoholic Fatty Liver Disease (NCT04881760)
This Phase 2A clinical trial was a sub-study of the Phase 2 clinical trial in obesity mentioned earlier, done for the purpose of measuring changes in liver fat and other associated biomarkers within people suffering from metabolic dysfunctionassociated steatotic liver disease (MASLD).
(NOTE: MASLD and NAFLD are used interchangeably due to a recently updated naming and diagnosis criteria of fatty liver disease)
Test Subjects (n = 98):
- Mean age = 46.6 years
- Mean weight = 110.2 kg
- Mean BMI = 38.4 kg/m²
- >10% liver fat content as determined by a magnetic resonance imaging proton density fat fraction (MRI–PDFF) scan
Dosing Schedule:
- Patients were randomly assigned to the following groups for 48 weeks
- Group #1 = Placebo
- Group #2 = 1.0mg Retatrutide injected subcutaneously once a week
- Group #3 = 4.0mg Retatrutide injected subcutaneously once a week
- Group #4 = 8.0mg Retatrutide injected subcutaneously once a week
- Group #5 = 12.0mg Retatrutide injected subcutaneously once a week
Clinical Outcomes:

- Relative mean change in liver fat from baseline after 48 weeks (%)
- Placebo = -4.6%
- 1mg Retatrutide = -51.3%
- 4mg Retatrutide = -81.7%
- 12mg Retatrutide = -86%
- Percentage of patients with liver fat content lower than 5% (indicating resolution of steatosis) after 48 weeks (%)
- Placebo = 0
- 1mg Retatrutide = 57
- 4mg Retatrutide = 89
- 12mg Retatrutide = 93
- Relative mean change in K-18, a marker of liver fibrosis, from baseline after 48 weeks (%)
- Placebo = -28%
- 1mg Retatrutide = -41%
- 4mg Retatrutide = -41.2%
- 12mg Retatrutide = -47.%
Side Effects:
- Identical to observations from the Phase 2 clinical trial on obese patients due to using a selection of its data, with no reports of liver toxicity
To wrap this study up:
- Higher doses of Retatrutide (8mg and 12mg) led to a reduction in liver fat of 70% or greater
- A “GGG” tri-agonist approach is the most effective for liver fat clearance, especially due to the addition of targeting the glucagon receptor alongside the GLP-1 and GIP receptors
- There was a strong association between weight loss, improved insulin sensitivity, better lipid metabolism, and liver fat reduction
- If it goes through further clinical trials, Retatrutide may be the first approved treatment for nonalcoholic steatohepatitis (NASH)
- Retatrutide poses a possible threat to the bottom line of liver transplant surgeons, similar to how BPC-157 and TB-500 are a competitive alternative to orthopedic surgeons and device manufacturers
Future Clinical Trials
As of this writing, the official Eli Lilly website states there are currently 11 clinical trials underway and 4 of them have already completed enrollment.
Most of them fall under the category of overweight/obesity or type 2 diabetes, but there’s a few I found by accident I think will be VERY interesting to see in the near future.
- A Phase 3 trial enrolling ~800 people for an 89-week study, where obese adults will be using either Retatrutide or Tirzepatide to see which peptide comes out as the winner
“A Study to Measure Calorie Consumption and Usage in Participants With Obesity Using LY3437943”
- A Phase 1 trial enrolling ~74 obese adults for a 6-month study, where Retatrutide will be examined for its effects on energy intake, energy expenditure and appetite when compared against a placebo
- A Phase 2 trial enrolling ~120 people for a 31-week study, where obese/overweight adults with chronic kidney disease (CKD) and/or Type 2 Diabetes will use Retatrutide to assess its effects on renal function
The Best Retatrutide Dose For Maximal Fat Loss, Appetite Suppression, And Lean Muscle Preservation

I’ve kept you waiting long enough with all the boring science mumbo-jumbo.
Let’s roll up our sleeves and talk about the absolute best way to use Retatrutide, along with what you can expect on your first right with this groundbreaking peptide.
I AM going to start by mentioning my own personal journey as it will explain why my recommendations stand as they are.
Most People Will End Up Overdosing Retatrutide
My very first discovery of Retatrutide dates back to the end of 2022.
I was so taken aback by the jaw-dropping preclinical results that I shared them with my audience in my flagship article about the best peptide stacks.
It was good enough to get a feature in my book Optimize Your Health With Therapeutic Peptides.
Around this time, I was still gung-ho on Tirzepatide as the world’s best molecule for easier and faster fat loss via its powerful appetite suppression properties.
And I was writing 30 Days 2 Shredz for release in September 2023, I looked for every possible way to get my hands on Retatrutide so I could come up with a viable contest prep protocol before the book was released.
Once the results from the Phase 2 clinical trial investigating Retatrutide in obese people were made public in June 2023, I KNEW the entire biohacking industry would see it as a coveted treasure.
So I asked for a giant favor from a very good friend a walking behemoth in both the peptides and research chemical vendor spaces.
After spending a lot of cash and countless hours digging up research on peptide synthesis, he was able to personally deliver a few precious vials of Retatrutide to my house.
From there, I spent the next 6 weeks experimenting with a dose of 2mg injected subcutaneously once per week.
By the end of August 2023, I had experienced and seen enough.
Here’s what I noticed at first:
The appetite suppression offered by Tirzepatide with dramatically enhanced fat loss via metabolic uncoupling and increased thermogenesis while at rest.
Outside of smaller bowel movements, no side effects were experienced on my end.
So for the next two weeks, I then upped the dose to 3mg per week.
Notice how we obey the law of “Start low and go up slow”, and NOT the “start high, go even higher” quackery performed by most prescribing doctors.
This is a rookie-level mistake still being made with Semaglutide and Tirzepatide, and it won’t surprise me to see this idiocy continue to happen once Retatrutide is FDA-approved.
By far, failing to start at a tolerable dose and maximize its effects (while only moving up when necessary) is the #1 reason why people get nasty side effects from GLP-1 peptides.
And it’s a good thing I followed my own advice.
Because adding in just an extra milligram led to dramatically enhanced sweating (even while standing still) and an enhanced resting metabolic rate.
But there was something else that happened… due to calories being burned at such a ridiculous rate, my hunger was through the roof.
The imposed metabolic demand by the one dose of Retatrutide made me RAVENOUS for everything and anything around me.
(NOTE: While Retatrutide itself has not been directly studied for its effects on energy expenditure, the medical literature shows glucagon infusions on its own can increase it in humans… all the more reason you should pay attention to the Phase 1 clinical trial measuring calorie consumption in Retatrutide users)
Gone was the appetite suppression, and in came the appetite elevation.
My solution to this problem was simple:
1 shot of 2.5-5 mg of Tirzepatide weekly combined with 1 shot of Retatrutide at 2-4 mg weekly
By leveraging the appetite-suppressing effects of Tirzepatide to eliminate cravings and hunger, I was able to get the best of both worlds simultaneously.
The Power Of Microdosing Retatrutide
When 2024 came around, several discussions with my private inner circle prompted me to do something radically different.
Instead of adhering to the limited thinking behind weekly injections, I was curious to see what would happen if I divided my already small dose of Retatrutide into 3-4 microdoses throughout the week.
I did this for a few reasons:
- Yes, Retatrutide’s world-changing results came from using the highest dose possible… but from what I saw and heard, taking a big dose at the start of the week made life unbearable for a lot of people
- A lean individual, let alone someone at a normal weight, will literally collapse from being overwhelmed by the sheer power of a Retatrutide dose meant for insulin-resistant dumpster fires (even if they work their way up to the dose gradually over time)
- 2-3mg of Retatrutide was already a *decent level* and I had no desire to use more, so the smart play was to lower the dose to understand if improving my results was possible
- For the inflamed dumpster fires, splitting the dose into smaller pieces might be the trick to greater adherence
So I settled on what I now believe is the best microdosing Retatrutide protocol if you’re using it solo:
0.25-0.5 mg injected subcutaneously 3 days a week, with ~48 hours in-between injections (ex. Monday, Wednesday, Friday)
You’re still putting a blowtorch to your metabolism without wanting to stuff your face silly, which comes in handy when you’re in a cutting phase.
If anything, you’ll find your appetite and cravings are suppressed at just the right amount; not too much to the point where eating one bite leaves you nauseous.
Plus there’s this awesome boost in energy levels you get, where you can stay focused for far longer without getting fatigued.
If you’re following an alternate-day fasting protocol like I am, Retatrutide is best used on your non-training days.
Other Retatrutide Stacks You MUST Use
These are some ungodly combinations I’ve personally experimented with to get the best out of Retatrutide.
Retatrutide + SS-31 For Smashing Through Walls (And Prs)
- The SS-31 peptide helps optimize mitochondrial health, but in combination with Retatrutide it makes a world of difference in your peak physical performance in the gym
- Retatrutide: 0.15-0.50mg injected subcutaneously every-other-day, ideally on fasting days
- SS-31: 250-300mcg injected subcutaneously alongside Retatrutide on fasting days
Retatrutide + Calocurb For Anabolic Appetite Suppression
- The higher dose of Retatrutide makes it easier to stay in the caloric surplus necessary to build muscle, but Calocurb helps you feel full at just the right time (i.e. you hit your caloric surplus feeling satisfied, instead of wolfing down 500-100 extra calories)
- Retatrutide: 2mg injected subcutaneously once a week
- Calocurb: 3-4 capsules once per day at the same time as Retatrutide, possibly twice after 4 hours for further elimination of hunger.
Retatrutide + SLU-PP-332 For Extremely Aggressive Fat Loss
- Monica and I added SLU-PP-332 on top of Retatrutide when we were preparing for a photoshoot – no diuretics, no larb, no photo editing, NOTHING. Easiest and most successful cut of my life. SLU-PP-332 adds additional nutrition partitioning and increased thermogenesis to give you “Retatrutide on steroids”
- Retatrutide: 0.15-0.50mg injected subcutaneously every-other-day, ideally on fasting days
- SLU-PP-332: 1000-2000mcg per day (first thing in the morning while fasted around 30 minutes before resistance/cardio training, then again 90 minutes after lunch

CONCLUSION: The God-Tier GLP-1 Peptide Of The Decade (So Far)

Out of all the wonderful things I could name about Retatrutide, the best one is how it equally benefits both the fully optimized and the fully sick among us.
Obese and insulin-resistant people will discover Retatrutide helps them get rid of unwanted belly fat much faster while re-wiring a dysfunctional relationship with food and their body’s hunger signals caused by decades of neglectful damage.
Bodybuilders and biohackers will no longer equate shredding down to single-digit body fat as ‘miserable’ — we can finally get rid of the old idea that contest prep and staying super-lean year-round has to feel like torture.
Long-term sustainable weight loss, whether returning to normalcy or seeking godhood, is no longer a pipe dream.
Gone are the days when your monkey mind nags you relentlessly to have a few extra cookies.
Retatrutide puts you back in the driver’s seat of your biology.
If you’re FINALLY read to make the leap and start using Retatrutide for yourself, pay close attention:
BioLongevity Labs sets the benchmark for USA-manufactured research peptides, with a relentless focus on purity, stringent third-party testing, and top-notch customer service.
We consistently deliver the highest quality products, trusted by professionals for both personal and clinical use.
Whether you’re looking to elevate your performance or integrate these products into research applications, BioLongevity Labs is THE most trusted source you can count on.

Use code JayC to get 15% off your order!
When you’re ready to take your Retatrutide journey to the next level, I invite you to join my Fully Optimized Health Private Membership Group.
You’ll get exclusive access to cutting-edge protocols, expert insights, and a community of high-performers committed to living their best lives.
Now, if you want to take your health optimization journey to the next level…
You’ll have to dive deeper into using peptides to optimize health, especially if you’re in your 30s and beyond.
And in doing so, you’ll unlock cutting-edge biohacking intel and the latest and greatest in elite health optimization strategies.
If that sounds like you, don’t forget to check out our other premium educational content dedicated to helping you fully optimize your health:
Peptides Demystified – the step-by-step, A-to-Z system for newbies desiring to master peptide use for the first time and forever.
The Ultimate GLP-1 Video Masterclass – how to PROPERLY utilize the world’s most powerful weight loss drugs for enhanced fat loss and overall longevity.
The Modern Woman’s Peptide Course – a must-have resource for any woman seeking to become more feminine, sexier, leaner, and healthier through the use of peptides.
Life Enhanced – Unlock the secrets to TOTAL Mind-Body-Spirit Optimization as Hunter Williams and I teach you how to live at the tip of the spear.
30 Days 2 Shredz – Reprogram Your Mind and Body for Maximum Fat Loss in Minimum Time with our Optimized Fasting Protocol
See you on the inside!
An remember:
Raise Your Vibration To Optimize Your Love Creation!